
Talk:Myalgic encephalomyelitis/chronic fatigue syndrome/Archive 20
| This is an archive of past discussions about Myalgic encephalomyelitis. Do not edit the contents of this page. If you wish to start a new discussion or revive an old one, please do so on the current talk page. |
| Archive 15 | ← | Archive 18 | Archive 19 | Archive 20 | Archive 21 | Archive 22 | → | Archive 24 |
External links modified
Hello fellow Wikipedians,
I have just modified 2 external links on Chronic fatigue syndrome. Please take a moment to review my edit. If you have any questions, or need the bot to ignore the links, or the page altogether, please visit this simple FaQ for additional information. I made the following changes:
- Added archive https://web.archive.org/web/20100918150632/http://cfids-cab.org/cfs-inform/CFS.case.def/carruthers.etal03.pdf to http://www.cfids-cab.org/cfs-inform/CFS.case.def/carruthers.etal03.pdf
- Corrected formatting/usage for http://www.iacfsme.org/PACETrial/tabid/450/Default.aspx
When you have finished reviewing my changes, you may follow the instructions on the template below to fix any issues with the URLs.
This message was posted before February 2018. After February 2018, "External links modified" talk page sections are no longer generated or monitored by InternetArchiveBot. No special action is required regarding these talk page notices, other than regular verification using the archive tool instructions below. Editors have permission to delete these "External links modified" talk page sections if they want to de-clutter talk pages, but see the RfC before doing mass systematic removals. This message is updated dynamically through the template {{source check}} (last update: 5 June 2024).
- If you have discovered URLs which were erroneously considered dead by the bot, you can report them with this tool.
- If you found an error with any archives or the URLs themselves, you can fix them with this tool.
Cheers.—InternetArchiveBot (Report bug) 23:32, 6 August 2017 (UTC)
Aspro's edits
I don't follow Aspro's logic. Why is the ICD10 relevant for removing the psychiatry specialty when ICD classifies CFS under R53.82, which is unspecified cause? The original edit was in error because CFS is only classified under 93.3 when it is post-viral. Also, you removed the Psychological section under pathphysiology with no explanation. (It was removed in error in Jan, and I just re-added it). --HotSection (talk) 20:30, 7 September 2017 (UTC)
- Aspro's logic is that 'if' R53.82 included psychiatric it would state that – which it doesn’t. OK, so you new here but don't revert declined edits by review editors . Also Wessely is now thoroughly discredited as he unilaterally altered the UK ICD database to included a psychiatric comorbidity without authority. So that section on is going again as well, because it was justly removed. Aspro (talk) 22:16, 8 September 2017 (UTC)
- The point is that R53.82 is neutral about cause. R53.82 has nothing whatsoever to say about whether or not CFS is part of psychiatry. Also, I don't see that you're a review editor, and I'm pretty sure that newbies are allowed to revert edits here. Anyway, you still haven't given any reasons for removing those edits, other than your own bias against psychiatry (which, needless to say, isn't a good reason for removing them). There is more than sufficient evidence to include those edits, not least of which are the references in the section itself. --HotSection (talk) 22:23, 8 September 2017 (UTC)
- I see once again you've reverted that info without any justification. I'd strongly suggest that you re-add it. You can't just remove sections from wikipedia without justification (although you should know that, being a long-time editor here). --HotSection (talk) 22:26, 8 September 2017 (UTC)
- ? I am I so biased against psychiatry that you think I was just suffering a momentary psychotic episode when I created [Hanwell Asylum] which is an article in praise of psychiatry? A former school friend or two or three an some later acquaintances are only alive today because of the expert help they received during moments of crisis. I have also, put in many hours of voluntary work ( at the for said St. Bernard's Hospital Aka Hanwell Asylum ) – which lead me to create the article and contribute to other articles, etc. So your unfounded accusation against me does not get off the starting block. The point is that Wikipedia is not a paper encyclopedia, so it it easy to keep current – but you are adding back, old and out of date stuff. By all means create a section on former hypothesis but don't add them back as being the current state of knowledge. Just as some who have had their lives dramatically changes by physical injuries from say accidents or encounters with IED etc., may benefit from some form of physiological therapy, it doesn’t follow that they suffer mental disorders (ie psychiatric) either. Likewise, those who have had their lives dramatically changed by CFS may benefit from some coping therapies also but not because they have a metal disorder either. Wessely et. al. is old hypothesis which did didn’t stand up to later scrutiny., The causes of CFS is now recognized as physiological and not incorporating a mental disorder. So we don't need any of this old stuffs added back unless it is for the purposes of historic context. Aspro (talk) 12:54, 10 September 2017 (UTC)
Causes
The article currently references a review from 2003 which concluded that "Genetic, physiological and psychological factors are thought to work together to precipitate and perpetuate the condition" [1]. This phrase is problematic because it sounds like consensus view but isn't. It also overstates the existing evidence: there is only tentative evidence that psychological factors cause or perpetuate the illness (a review of risk factors cited later on the page concluded that definitive evidence that is meaningful for clinicians is lacking [2]). Just like infectious causes, psychological causes have been proposed but are not proven. The 2015 review by the US National Academies of Medicine rejected the view that the illness is caused by psychological factors: [3], so clearly the panel did not believe that psychological factors cause and perpetuate the illness. Abmayer (talk) 20:25, 13 September 2017 (UTC)
- We also say "Biological, genetic, infectious, and psychological mechanisms have been proposed, but the cause is not understood." Doc James (talk · contribs · email) 21:59, 13 September 2017 (UTC)
Undo of revision 800670227
@Petergstrom: Can you explain why you undid revision 800670227? The revised phrasing ("some patients and clinicians") is an articulation more consistent with the cited source Frumkin H, which does not make the claim that all (or even any) sufferers or clinicians find this term "offensive." Rather, the authors use the adjective "derisive" in a context that is clearly intended as an expression of their (the authors') own opinion and not part of a factual assertion about views held by broad groups like patients or clinicians. 69.145.80.162 (talk) 00:31, 15 September 2017 (UTC)69.145.80.162
- @69.145.80.162: The source also stated Yuppie flu "maligned" patients, was "pejorative" as well as "derisive". If you also look at news archives in Google for the term used in the last 10-15 years it explains how the term is inaccurate and contributed to misunderstanding and distress of patients and providers. Broad groups like patients and clinicians is specified or implied by language used in the cited and other sources. [1] Ward20 (talk) 06:20, 15 September 2017 (UTC)
Post-exertional malaise (PEM) is now a primary symptom required for diagnosis
As mentioned by Aspro in Talk:Chronic_fatigue_syndrome/Archive_19#New_CDC_Guidance:_Post-Exertional_Malaise_.28PEM.29_is_now_a_Primary_Symptom_required_for_diagnosis post-exertional malaise (PEM) is now a primary symptom required for diagnosis in the CDC guidance. https://www.cdc.gov/me-cfs/symptoms-diagnosis/symptoms.html . I am going to add it to the Symptoms in the side bar. C7762 (talk) 09:11, 22 September 2017 (UTC)
@Doc James: Please do not change "post-exertional malaise (PEM)" to "feeling tired after exercise" without first discussing it here. The CDC website clearly states that :- 1. it is named Post-exertional malaise (PEM). 2. it involves a worsening of many symptoms, not just fatigue. 3. it is caused exertion of any type of activity (physical or mental). 4. it is a primary symptom required for diagnosis. 5.'feeling tired after exercise' is a broad and incorrect description that is not mentioned in the text.
"Worsening of ME/CFS symptoms after physical or mental activity that would not have caused a problem before illness. This is known as post-exertional malaise (PEM). People with ME/CFS often describe this experience as a “crash,” “relapse,” or “collapse.” It may take days, weeks, or longer to recover from a crash. Sometimes patients may be house-bound or even completely bed-bound during crashes. People with ME/CFS may not be able to predict what will cause a crash or how long it will last."
C7762 (talk) 23:20, 22 September 2017 (UTC)
- We write the lead and especially the infobar in easy to understand language. That is the point of it. Latin can go in the body. There is nothing wrong with translating Latin into English. When there is an article on post exertional fatigue we can link the easier to understand language to it.
- Have adjusted to "worsening of symptoms with activity" to better match the definition above. Doc James (talk · contribs · email) 23:21, 22 September 2017 (UTC)
- Few additional things (1) we do not link to disambig pages (2) refs go after punctuation not before. Doc James (talk · contribs · email) 23:26, 22 September 2017 (UTC)
@Doc James: Thanks. C7762 (talk) 23:30, 22 September 2017 (UTC)
- That wording works for you User:C7762? Doc James (talk · contribs · email) 23:36, 22 September 2017 (UTC)
User: Doc James Yes, it is a better description of the CDC definition. Thanks. I will look at creating a new page to describe it based on the CDC text then it can be linked to. C7762 (talk) 23:41, 22 September 2017 (UTC)
NICE CFS Guidelines to be updated
Should edits be made to reflect that NICE are to update its CFS guidelines. One of the reasons for the decision is :-
"Key trials (particularly PACE [Pacing, graded Activity, and Cognitive behaviour therapy; a randomised Evaluation], but also Cochrane reviews of CBT and GET) have been criticised for inflating the efficacy of interventions. Issues include that some studies only require fatigue in the case definition, which may incorporate other fatiguing conditions with the potential to complicate results."
C7762 (talk) 19:10, 20 September 2017 (UTC)
Made edit. C7762 (talk) 09:26, 22 September 2017 (UTC)
OK C7762 (talk) 23:43, 22 September 2017 (UTC)
ICD-10 code
I've just gone to add the ICD-10 code to this article, when I saw that it was already there (along with ICD-9-CM codes). However, the parameters are set to iCD instead of ICD. Couldn't see why this might have been done on the last 500 revisions; but thought I'd best check as it seems deliberate? Little pob (talk) 19:56, 29 September 2017 (UTC)
Should this page follow example of "The Lightning Process" Page and reference research with out WP:MEDRS sources?
I propose this page follows the example of The_Lightning_Process page and no longer require the use of sources meeting WP:MEDRS requirements. Following the example of The_Lightning_Process Press releases, Blogs and Original research papers should be permitted as sources on this page.C7762 (talk) 14:15, 5 October 2017 (UTC)
- As discussed on the LP page, the only reason we are doing that is because nothing else is available, and we've put a lot of caveats in. This is how it works in other articles, like the one on liberation therapy/CCSVI, and it doesn't actually fail MEDRS. I'd suggest discussing this on the LP page, where the discussion belongs. --sciencewatcher (talk) 14:42, 5 October 2017 (UTC)
I am simply proposing we follow the example set by the The_Lightning_Process page. Surely the the same logic can be applied to this page: If MEDRS sources are not available we can use whatever is available such as press releases or blogs. As you said sciencewatcher the same logic is applied to other pages such as liberation therapy/CCSVI, why not here? C7762 (talk) 15:44, 5 October 2017 (UTC)
- For CFS we do already have many high quality reviews. For CCSVI and LP we don't. We did use an exception here for XMRV, where we included it with just one single study due to its importance, as I'm sure you already know (if not, check the page history). Is there any important treatment for CFS that has just a single trial that you're thinking of including? The only other one I can think of is rituxamib, but we do already include it here on the treatment page. So I'm a bit baffled as to what you're actually proposing. --sciencewatcher (talk) 16:12, 5 October 2017 (UTC)
- We use the best avaliable sources. I have trimmed a number of things at Lightning Process.
- We sometimes bend things a bit in the research section for primary sources. Doc James (talk · contribs · email) 18:20, 5 October 2017 (UTC)
Thanks for the clarification on MEDRS. C7762 (talk) 11:09, 11 October 2017 (UTC)
Risk factors
Aspro, can you point out where pmid 12562565 says that physical attributions "do not seem a risk factor for the development of CFS"? The source says " it has been suggested that somatic attributions may be a risk factor for the development of chronic fatigue syndrome " which is almost the opposite of your edit. --sciencewatcher (talk) 19:18, 6 October 2017 (UTC)
- Yup and the other bit of that sentence is supported by "Patients' perceptions, attributions, and coping skills, however, may help perpetuate the illness." Doc James (talk · contribs · email) 22:52, 6 October 2017 (UTC)
- This was published in 2003 when lacking a good psychological explanations, psychiatric explanations were all the rage. Believe it or not, a few psychiatrists were suggesting people where sick because they thought that they where sick. A decade and a half later, one has to question what value this ref gives? Whether biblical Jesus existed or not, it was well understood that a lame man, could at times roll up his bed and walk ( akin to placebo when delivered by the power of the word), But if his lameness was do to say polio, then all the scriptures in the bible would not make him whole again. There are also some US faith healers that claim, that at their meetings they have brought about miraculous cures (by the power of the word) – but independent follows ups have never been able to support those claims. To make more clear. Wikipedia:What_Wikipedia_is_not#Wikipedia_is_not_a_paper_encyclopediaWP is not a paper encyclopedia and so can be kept up to date with current wisdom. A 14 year old and discredited line of hypotheses ( read the research done since) and has no place on 2017 WP. No more than the hypothesis for bad air (malaria. Italian, contraction of mala aria or bad air ). Nor that all peptic ulcers (as psychiatrist claimed) were caused by stress until Barry Marshall unequivocally demonstrated otherwise. What is of value to a patient is effective treatment, rather than ineffective hyperbole. This is the essence of why doctors go through years of training in order that the can perform in the best way that they know how. In the late 1960's early1970's, what with man landing on the Moon, many editors of this generation after me, are too believing in what is only too obvious to them. Yet , these hypothesis's have not place here anymore. This ref has been linked to in the article 9 times which in 2017 is nine times too many. Aspro (talk) 14:55, 15 October 2017 (UTC)
Removal of text
We had a RfC here about this text "Evidence suggests that cognitive behavioral therapy and a gradual increase in activity suited to individual capacity can be beneficial in some cases.[4][5] In a systematic review of exercise therapy, no evidence of serious adverse effects was found; however data was insufficient to form a conclusion.[5]"
Despite this User:Broookss continues to remove it which is getting disruptive. Doc James (talk · contribs · email) 05:41, 15 October 2017 (UTC)
- This information is out of date. The RfC is from Jan 8, 2017 which predates the removal of GET and CBT from the CDC website and predates the special issue of the PACE trial from the Journal of Health Psychology. [6] This text is not consistent with the current science, which is that GET and CBT are harmful to ME/CFS patients. [7] [8] — Preceding unsigned comment added by Broookss (talk • contribs)
- How about the Journal of Health Psychology: "Cognitive behavioural therapy may bring about changes in self-reported fatigue for some patients in the short term, however there is a lack of evidence for long-term benefit or for improving physical function and cognitive behavioural therapy may cause distress if inappropriately prescribed." and Socialmedicinsk tidskrift: "Surveys suggest that the efficacy of CBT is no better than placebo and that GET is harmful. Therefore, cognitive behavioral therapy and graded exercise therapy for ME/CFS are not evidence based.". Gaia Octavia Agrippa Talk 18:53, 17 October 2017 (UTC)
- Broookss's makes a good point about the the CDC website being updated. Currently national treatment guidelines for the U.S. (CDC) and the UK (NHS) are quite different. We should mention that there are varying sets of treatment recommendations. And given that the CDC does not mention CBT or GED in its treatment guidelines, I don't think they belong in the infobox. I would rather leave the Treatment parameters of the Infobox blank. To put the CDC's omission of CBT and GED into perspective, their page mentions even acupuncture as being possibly helpful, for heaven's sake. We might want to stop and ask ourselves if Wikipedia should recommend treatments that the CDC considers less recommendation-worthy than acupuncture. Clayoquot (talk | contribs) 19:48, 17 October 2017 (UTC)
- Right now the info for clinicians page just says "new info coming end 2017" so I don't think we can conclude much yet. There is a quote from the CDC here saying why they removed that info. They do still support exercise, but many doctors incorrectly interpreted it as "go to the gym", so it sounds like they're just in the process of rewriting it so that it has appropriate cautions. --sciencewatcher (talk) 22:56, 17 October 2017 (UTC)
- The fact that page X is due to be updated doesn't mean we can't conclude much yet from page Y. If the CDC doesn't want people to conclude things from reading a page, they don't publish the page at all. That article is interesting though in that it says that the NHS guidelines are going to be reassessed, which should lead us towards giving the NHS guidelines less weight. Clayoquot (talk | contribs) 05:45, 18 October 2017 (UTC)
- This discussion is why I edited[3] the lead section to be a general description, and that there are various beneficial symptomatic treatments that can be used as management strategies. CBT and exercise therapy are part of these treatment strategies for symptoms. The reviews state the data for CBT and GET therapies show no benefit for many ME/CFS symptoms. Another reason to change the lead is that housebound or bed bound persons with ME/CFS are not included in CBT or GET studies so benefits or harms in this group are unknown. As I recall, 25% of persons with ME/CFS are housebound or bed bound sometime during their illness. Exposing this group to CBT or GET is reckless. Leave Specific treatment information in the treatment section so complexities and controversies can be better explained there. The lead, the way it presently exists, does not adequately describe there are many supportive symptomatic treatments available for ME/CFS. Ward20 (talk) 01:00, 18 October 2017 (UTC)
We state "Evidence suggests that cognitive behavioral therapy and a gradual increase in activity suited to individual capacity can be beneficial in some cases"
This is based on this 2015 review in the Annals of Internal Medicine[4]. Annals of Internal Medicine has an impact factor of 17.2. Ref says "Counseling therapies and graded exercise therapy compared with no treatment, relaxation, or support improved fatigue, function, global improvement, and work impairment in some trials; counseling therapies also improved quality of life (low to moderate strength of evidence)."
and
This 2016 review by Cochrane [5]. Cochrane has an impact factor of 6.6. It says "Patients with CFS may generally benefit and feel less fatigued following exercise therapy, and no evidence suggests that exercise therapy may worsen outcomes."
"Journal of Health Psychology" has an impact factor of 1.8.
Doc James (talk · contribs · email) 09:39, 18 October 2017 (UTC)
- So what does the CDC currently recommend:
- a) "Light exercise and stretching earlier in the day, at least four hours before bedtime, might improve sleep."
- b) "Talking with a therapist to help find strategies to cope with the illness and its impact on daily life and relationships."
- c) "Avoiding ‘push-and-crash’ cycles through carefully managing activity."
- None of those statements contradicts the use of either CBT or GET. We have some who appear to be attempting to read more into what the CDC wrote than what is actually their. Doc James (talk · contribs · email) 09:51, 18 October 2017 (UTC)
- The RFC was a good tool for the question it was framed to answer, which was what to say about GET. It was not framed to answer the question of what to say about CFS treatment as a whole, which is the question that the lead and infobox have to answer. When I look at the treatment guidelines from the NHS and the CDC, the aspects that they give the most weight to are that treatment consists of symptom management, and that doctors, patients, and families should work together to create an individualized treatment plan. Ward20's wording summed this up well: "Illness management by treating the most burdensome CFS symptoms with supportive care may help alleviate patient distress and improve quality of life." The part that bugs me the most is the infobox, because it gives the impression that GET and CBT are "the" treatments. Would anyone object to changing the infobox to say Treatment = Symptomatic, as we do in the Common cold infobox? Clayoquot (talk | contribs) 06:37, 19 October 2017 (UTC)
- Treatment is more than just symptomatic here. So yes I would object. This change IMO is overly vague[6] Doc James (talk · contribs · email) 11:40, 19 October 2017 (UTC)
- Which treatments are more than just symptomatic? GET or CBT or both? Clayoquot (talk | contribs) 19:17, 19 October 2017 (UTC)
- What I meant to say is what we have now is more than simple saying treatment is symptomatic. Doc James (talk · contribs · email) 22:20, 19 October 2017 (UTC)
- Which treatments are more than just symptomatic? GET or CBT or both? Clayoquot (talk | contribs) 19:17, 19 October 2017 (UTC)
- Treatment is more than just symptomatic here. So yes I would object. This change IMO is overly vague[6] Doc James (talk · contribs · email) 11:40, 19 October 2017 (UTC)
- The RFC was a good tool for the question it was framed to answer, which was what to say about GET. It was not framed to answer the question of what to say about CFS treatment as a whole, which is the question that the lead and infobox have to answer. When I look at the treatment guidelines from the NHS and the CDC, the aspects that they give the most weight to are that treatment consists of symptom management, and that doctors, patients, and families should work together to create an individualized treatment plan. Ward20's wording summed this up well: "Illness management by treating the most burdensome CFS symptoms with supportive care may help alleviate patient distress and improve quality of life." The part that bugs me the most is the infobox, because it gives the impression that GET and CBT are "the" treatments. Would anyone object to changing the infobox to say Treatment = Symptomatic, as we do in the Common cold infobox? Clayoquot (talk | contribs) 06:37, 19 October 2017 (UTC)
- (Edit conflict with Ward20 below) Sorry Doc James, I'm still having trouble reading your handwriting ;) Where is "what we have now"? And are you saying that CBT and GET need to be in the infobox? Clayoquot (talk | contribs) 05:37, 20 October 2017 (UTC)
- @Clayoquot: per my discussion below I agree the infobox should say Treatment = Symptomatic. Ward20 (talk) 05:53, 20 October 2017 (UTC)
- I disagree, CBT and GET treatments don't have enough weight to be in the lead because they are only treatments for certain symptoms mostly in a subset of patients. The CDC and NHS first emphasize treating symptomatically the most distressing symptoms. CDC:("Patients, their families, and healthcare providers need to work together to decide which symptom causes the most problems. This should be treated first")[7]. NHS:("1.4.1 Symptom management")[8]. This supports wording similar to my edit. [9]
- From the Annals review[10], "...a debilitating multisystem condition characterized by chronic and disabling fatigue and several other symptoms, including pain, sleep disturbance, neurologic and cognitive changes, motor impairment, and altered immune and autonomic responses...postexertional malaise and memory or concentration problems to be critical components." Discussion:,"Counseling, behavior therapies, and GET improved measures of fatigue, function, global improvement, and work impairment; counseling and behavior therapies also improved quality of life (low to moderate strength of evidence)". Not all symptoms improved.
- Additionally, the Annals review authors warned:
- "This systematic review was limited by deficiencies of the trials. Most trials enrolled participants on the basis of case definitions for CFS only. The Oxford CFS case definition is the least restrictive, and its use as entry criteria could have resulted in selection of participants with other fatiguing illnesses or illnesses that resolve spontaneously with time"
- The Annals review[11] was published in 2015. The same authors published a 2016 addendum[12] to the original 2014 review[13] the Annals review was based upon, in order to assess the impact of the Oxford criteria studies by removing the Oxford data. For CBT, the result was a low strength of evidence for decreased fatigue, and no evidence of benefit for any other parameter. For GET, there was, "insufficient evidence of the effectiveness of GET on any outcome." Further evidence CBT and GET do not belong in the lead.
- Rintatolimod does not have any weight for being in the lead because it is only documented to be in use at a few experimental sites in the US with very few persons.
- Sorry to have a late reply due to RL. Ward20 (talk) 05:18, 20 October 2017 (UTC)
- Have added that treatment is symptomatic. Disagree with the rest of what you have writtenDoc James (talk · contribs · email) 16:52, 20 October 2017 (UTC)
- There is a difference in opinion from CDC and NICE here. CDC says treatments are for symptoms, whereas NICE says CBT and GET are for treating the illness itself. (It talks about addressing perpetuating factors, so clearly it's more than just symptom control). Also it talks about using alternative therapies and pharmacological interventions for symptom control, but doesn't say that for CBT and GET. Also, given that the most of the CBT and GET studies use a cognitive behavioural model, that would seem to contradict the statement that they are mainly intended for symptom control. --sciencewatcher (talk) 17:32, 20 October 2017 (UTC)
- Those are good points, but the NICE page says "Is this guideline up to date? We checked this guideline in September 2017 and we are updating it.". If you click on that link and read further you see that NICE is planning a full update of the guideline with modified scope, because "a large volume of new evidence since 2007 needs to be incorporated." I don't think we should be using the 2007 NICE guidelines as an up-to-date reliable source. The 2017 CDC guidelines should be given more weight. Clayoquot (talk | contribs) 20:49, 20 October 2017 (UTC)
(out)I think the new changes are a reasonable compromise, and IMO the symptomatic treatment addition alone improves the article. I understand that CBT and GET is based upon a behavioral theory for ME/CFS, but in reality the reviews state that these treatment studies have been biased to the Oxford criteria patient subset and that influences the study data. The new reviews are recognizing this, calling for new studies to strictly define the enrolled populations. This should reduce the conflicting data among future studies and make editing the ME/CFS article less problematic. The editing in this article can't anticipate how the NHS guidelines are going change either. If NICE sticks to schedule maybe there will be some clarification of their position this year that can be incorporated. Until then there is still a lot of material in the article that relies on older reviews and obsolete links. I don't anticipate short term major changes to the article but there is still a lot to do to tweak the material to reflect the newest high quality sources. Doc James has been working diligently to accomplish this task. Ward20 (talk) 07:52, 21 October 2017 (UTC)
- Treatment is sort of divided into curative and symptomatic / palliative. Will be interesting to see NICEs statements post update. Doc James (talk · contribs · email) 17:50, 21 October 2017 (UTC)
Classification of ME/CFS as a disease
The current version of the article lists ME/CFS as a "medical condition." This is not consistent with the science going back over 40 years. While there are many components to CFS, immune, neurological, and endocrine, ME/CFS is a neuroimmune disease and is officially classified as such. [9] ME/CFS has had this classification since 1969. [10] [11] — Preceding unsigned comment added by Broookss (talk • contribs)
Canvassing
We appear to have a patient advocacy group trying to change the page to their liking with comments including "Perhaps having a team would help." on reddit. Doc James (talk · contribs · email) 09:47, 18 October 2017 (UTC)
- I am not part of any advocacy group or 'team' but I have to ask why does it matter if a group of patients work on making changes as long as it meets the standards of Wikipedia? This is the only Illness that I am aware of where the patients are vilified (by the medical profession). This is a lazy method to suppress (valid) arguments and it would be a sad day if such tactics were used here. It should be noted that the narrative construct that CFS patients are extremists has been found to be untrue at a UK court. C7762 (talk) 13:36, 28 October 2017 (UTC)
- a perfectly acceptable observation by DJ. If patient advocacy groups start editing pages in violation of our community norms, they should expect to be held to account for not holding to them. Cfs/me advocacy groups are notorious for behaviour on the internet and irl for this mob handed behaviour, misinterpreting the known science and jumping the gun in many related area. Don’t worry about it, DocJames is just issuing a heads up to editors here, and Redditors. -Roxy the dog. bark 14:04, 28 October 2017 (UTC)
- I also wanted to mention that your comment above might be interpreted by extremely picky people as a legal threat, seeWP:NLT, which is strictly forbidden by our editing policy. I do not interpret it that way. I'd be interested in some sort of pointer to this interesting legal decision from the UK courts though. Can you point me? -Roxy the dog. bark 14:43, 28 October 2017 (UTC)
- a perfectly acceptable observation by DJ. If patient advocacy groups start editing pages in violation of our community norms, they should expect to be held to account for not holding to them. Cfs/me advocacy groups are notorious for behaviour on the internet and irl for this mob handed behaviour, misinterpreting the known science and jumping the gun in many related area. Don’t worry about it, DocJames is just issuing a heads up to editors here, and Redditors. -Roxy the dog. bark 14:04, 28 October 2017 (UTC)
- I am not part of any advocacy group or 'team' but I have to ask why does it matter if a group of patients work on making changes as long as it meets the standards of Wikipedia? This is the only Illness that I am aware of where the patients are vilified (by the medical profession). This is a lazy method to suppress (valid) arguments and it would be a sad day if such tactics were used here. It should be noted that the narrative construct that CFS patients are extremists has been found to be untrue at a UK court. C7762 (talk) 13:36, 28 October 2017 (UTC)
- I refer to the Upper Tribunal verdict involving the PACE trial data release. Where the verdict states there is that there was no evidence of claims of abuse or harassment by CFS patients (except for one incidence of heckling). Despite it being a main argument for not releasing the data.
- Roxy you state "CFS advocy groups are notorious". Firstly show the evidence (not opinion), secondly to dismiss the voice of a whole cohort because of a few bad apples is a lazy tactic to stop debate. If there is bad behaviour on this page then deal with it then, don't "Minority Report" the situation. C7762 (talk) 15:31, 28 October 2017 (UTC)
- I have no problem with my statement above, and frankly, couldn't care less what the Tribunal said in that regard. I have however formatted your post correctly with two extra colons. -Roxy the dog. bark 15:39, 28 October 2017 (UTC) -Roxy the dog. bark 15:39, 28 October 2017 (UTC)
- To summarize Roxy: You have a strongly held negative belief about a whole group of people for which you have no evidence and when presented with evidence that challenges your opinion you refuse to consider it. Nice. C7762 (talk) 16:41, 28 October 2017 (UTC)
- Just as your interpretation of the Tribunal report on the PACE trial is your own. I'm just warning fellow editors of my own, and many others, experiences. XMRV anybody? -Roxy the dog. bark 16:47, 28 October 2017 (UTC)
- The Tribunal Verdict is not my interpretation it is set out in black and white, Why not read it?. It was also reported in the UK press. I am sorry if you had a bad experience several years ago with XMRV but that is no reason to dismiss the input from a whole cohort C7762 (talk) 17:03, 28 October 2017 (UTC)
- I never said it was a bad experience. It was observation of typical CFS/ME victims and their behaviour on the internet and irl. The Tribunal based their verdict (Which I have read) on evidence presented to them about the PACE trial. Therefore, as you should know, Its verdict has no bearing on typically observed behaviour on the internet, and irl, by CFS/ME victims. You, and any Redditors and meatpuppets should be aware that Wikipedia will not allow such groups to move our article away from WP:NPOV -Roxy the dog. bark 17:13, 28 October 2017 (UTC)
- Roxy - I have no intention of moving your article away from WP:NPOV - I have been contributing to it for some time now. I am a little confused firstly you say "I'm just warning fellow editors of my own, and many others, experiences. XMRV anybody?" then "I never said it was a bad experience". If there has been bad behaviour from these "typical CFS/ME victims" on Wikipedia I am sure it was dealt with at the time and will be in the future. Maybe we should profile all potential contributors to this page.C7762 (talk) 18:18, 28 October 2017 (UTC)
- I never said it was a bad experience. It was observation of typical CFS/ME victims and their behaviour on the internet and irl. The Tribunal based their verdict (Which I have read) on evidence presented to them about the PACE trial. Therefore, as you should know, Its verdict has no bearing on typically observed behaviour on the internet, and irl, by CFS/ME victims. You, and any Redditors and meatpuppets should be aware that Wikipedia will not allow such groups to move our article away from WP:NPOV -Roxy the dog. bark 17:13, 28 October 2017 (UTC)
- The Tribunal Verdict is not my interpretation it is set out in black and white, Why not read it?. It was also reported in the UK press. I am sorry if you had a bad experience several years ago with XMRV but that is no reason to dismiss the input from a whole cohort C7762 (talk) 17:03, 28 October 2017 (UTC)
- Just as your interpretation of the Tribunal report on the PACE trial is your own. I'm just warning fellow editors of my own, and many others, experiences. XMRV anybody? -Roxy the dog. bark 16:47, 28 October 2017 (UTC)
- To summarize Roxy: You have a strongly held negative belief about a whole group of people for which you have no evidence and when presented with evidence that challenges your opinion you refuse to consider it. Nice. C7762 (talk) 16:41, 28 October 2017 (UTC)
Not my article. I shall not respond further. -Roxy the dog. bark 18:25, 28 October 2017 (UTC)
- There are a group of illnesses were some patient groups have tried to over interpret / misinterpret the evidence. Lyme is even more significant. Multiple sclerosis was another one with respect to the Liberation procedure (which liberated tax pays in Canada of millions of dollars).
- If people want to bring forwards recent reviews in major journals I, and I am sure others, are more than happy to look at them. This is not a silencing technique. This is more an emphasises that Wikipedia content is not determined by a vote. Doc James (talk · contribs · email) 20:36, 28 October 2017 (UTC)
Text
This was added "concluded that ME/CFS is a biologically based illness" but the source actually says "The cause or causes of ME/CFS remain unknown"[15] But also says "is a biologically based illness and proposed a new case definition and name (systemic exertion intolerance)" so will readd. Doc James (talk · contribs · email) 18:17, 26 September 2017 (UTC)
- @Doc James: In various places, why did you revert to older versions of text that cite CDC website as of 2011 or 2012? CDC launched an updated website for ME/CFS in July 2017. UsernameSasha (talk) 18:48, 26 September 2017 (UTC)UsernameSasha
@Doc James: OK, I see you have now made some additional interim edits that addressed at least some of the inaccuracies in the older versions of text citing to CDC (e.g., CDC's current website does not identify depression as a symptom). Will take a closer look at your edits.UsernameSasha (talk) 19:12, 26 September 2017 (UTC)
- Yes looking more closely much of it was good and I have added it back. Apologies. Doc James (talk · contribs · email) 19:15, 26 September 2017 (UTC)
There were two substantial additions by UsernameSasha (talk · contribs) [17] and [18] that were reverted by L3X1 and Doc James. Neither edit summary explains what's was wrong with the additions. Could you please explain? Clayoquot (talk | contribs) 07:26, 28 September 2017 (UTC)
- As mentioned above the source summarizes things by saying the cause is unknown. I am not sure a workshop represents an official position of the NIH. Also we should be summarizing not using large quotes.
- The bit on comparing how much money is spend on different diseases is primary research. The sources are not making that comparison. Doc James (talk · contribs · email) 16:05, 28 September 2017 (UTC)
- Thanks Doc James. There is a significant point of view that research on ME/CFS is underfunded. The part about the House Committee being "concerned that the level of funding is still very low considering the burden of disease" is one instance of this point of view. What is wrong with including that? W.r.t. comparisons, to satisfy WP:SYNTH, there needs to be a reliable source in which a comparison is made. Perhaps Sasha could point to such a source. Clayoquot (talk | contribs) 21:12, 28 September 2017 (UTC)
- My concern is that the source will it gives numbers does not make the comparison.[19] Not sure if there was another ref? Doc James (talk · contribs · email) 06:10, 29 September 2017 (UTC)
- The comparison is made by the Solve ME/CFS Initiative advocacy group here. Would that suffice to demonstrate that the comparison is not original research? Clayoquot (talk | contribs) 05:50, 3 October 2017 (UTC)
- We specifically try to avoid those sorts of sources. Doc James (talk · contribs · email) 05:00, 4 October 2017 (UTC)
- Doc James, I thought I had referenced a combo of appropriate sources to support the per patient funding comparisons, but maybe that was not clear by my placement of footnotes. By definition, it is not "primary research" to synthesize existing data on aggregate funding for a disease and figures on disease prevalence, in order to calculate a per patient funding estimate. The per patient funding comparisons are just a simple mathematical calculation comparing (1) aggregate funding amounts for specific diseases (ME/CFS, MS and HIV/AIDS), all taken from the same NIH report that sets forth a tabular comparison of such amounts by disease [20] to (2) reputable estimates on prevalence of such diseases. To give another example, if one was given the data that a box of 64 Crayola brand crayons cost $4.49, and a box of 48 off-brand crayons cost a buck at the dollar store, it would not be primary research to calculate cost/unit comparisons. If the footnoting or presentation of the data relating to these comparisons needs more clarity, I would appreciate additional guidance. Thanks! UsernameSasha (talk) 13:06, 15 October 2017 (UTC)
- You are correct that doing arithmetic to calculate per-patient funding is not primary research. However, usage of those figures to support a point of view is primary research unless someone else has made that argument first in a reliable source. I did some searching for sources on whether these figures have been used to argue for more research spending, and could not find a source other than the one above that Doc James rejected. I know that advocates for ME/CFS research do make this argument, and if we could source it appropriately I think it would be good to include. If not, we could and should include something along the lines of "The amount of funding allocated to CFS research in 2017 is X in the United States and Y in other countries. Patient advocates and some researchers believe research is significantly underfunded." It's easy to find sources for that. Clayoquot (talk | contribs) 23:08, 16 October 2017 (UTC)
- Have you cheked the CDC or NIH websites? There might be some press releases or info on their websites. --sciencewatcher (talk) 01:02, 17 October 2017 (UTC)
- I think mainstream news sources would also be fine, as we're talking about politics not biomedical information. Clayoquot (talk | contribs) 18:28, 17 October 2017 (UTC)
- This issue is one of primary research. A claim was trying to be made based on numbers that were not trying to make that claim. Doc James (talk · contribs · email) 20:40, 28 October 2017 (UTC)
- I think mainstream news sources would also be fine, as we're talking about politics not biomedical information. Clayoquot (talk | contribs) 18:28, 17 October 2017 (UTC)
- Have you cheked the CDC or NIH websites? There might be some press releases or info on their websites. --sciencewatcher (talk) 01:02, 17 October 2017 (UTC)
- You are correct that doing arithmetic to calculate per-patient funding is not primary research. However, usage of those figures to support a point of view is primary research unless someone else has made that argument first in a reliable source. I did some searching for sources on whether these figures have been used to argue for more research spending, and could not find a source other than the one above that Doc James rejected. I know that advocates for ME/CFS research do make this argument, and if we could source it appropriately I think it would be good to include. If not, we could and should include something along the lines of "The amount of funding allocated to CFS research in 2017 is X in the United States and Y in other countries. Patient advocates and some researchers believe research is significantly underfunded." It's easy to find sources for that. Clayoquot (talk | contribs) 23:08, 16 October 2017 (UTC)
- Doc James, I thought I had referenced a combo of appropriate sources to support the per patient funding comparisons, but maybe that was not clear by my placement of footnotes. By definition, it is not "primary research" to synthesize existing data on aggregate funding for a disease and figures on disease prevalence, in order to calculate a per patient funding estimate. The per patient funding comparisons are just a simple mathematical calculation comparing (1) aggregate funding amounts for specific diseases (ME/CFS, MS and HIV/AIDS), all taken from the same NIH report that sets forth a tabular comparison of such amounts by disease [20] to (2) reputable estimates on prevalence of such diseases. To give another example, if one was given the data that a box of 64 Crayola brand crayons cost $4.49, and a box of 48 off-brand crayons cost a buck at the dollar store, it would not be primary research to calculate cost/unit comparisons. If the footnoting or presentation of the data relating to these comparisons needs more clarity, I would appreciate additional guidance. Thanks! UsernameSasha (talk) 13:06, 15 October 2017 (UTC)
- We specifically try to avoid those sorts of sources. Doc James (talk · contribs · email) 05:00, 4 October 2017 (UTC)
- The comparison is made by the Solve ME/CFS Initiative advocacy group here. Would that suffice to demonstrate that the comparison is not original research? Clayoquot (talk | contribs) 05:50, 3 October 2017 (UTC)
- My concern is that the source will it gives numbers does not make the comparison.[19] Not sure if there was another ref? Doc James (talk · contribs · email) 06:10, 29 September 2017 (UTC)
- Thanks Doc James. There is a significant point of view that research on ME/CFS is underfunded. The part about the House Committee being "concerned that the level of funding is still very low considering the burden of disease" is one instance of this point of view. What is wrong with including that? W.r.t. comparisons, to satisfy WP:SYNTH, there needs to be a reliable source in which a comparison is made. Perhaps Sasha could point to such a source. Clayoquot (talk | contribs) 21:12, 28 September 2017 (UTC)
Are There Any Editors Paid by the Disability Insurance Industry to Work on This ME/CFS Article?
As is well known in the ME/CFS world, it is greatly in the interests of the disability insurance industry to make ME/CFS look as if it were an "all in the mind" disorder caused by psychogenic or biopsychosocial factors, rather than a disease with organic biological causes. This is because disability insurance rules generally stipulate that disability due to biological disease is covered for lifelong disability support payments where necessary, but disability due to mental health disorders are not covered for lifelong support. Thus the insurance industry can save billions in disability payouts if they make it appear that ME/CFS is an "all in the mind" mental disorder, rather than the organic biologically-caused disease that most scientific biomedical researchers view it to be. Indeed, the psychiatrists who have most promoted the idea that ME/CFS is an "all in the mind" biopsychosocial condition — people like Simon Wessely, and Prof Peter White — have been paid by disability insurance companies for their work, in spite of the obvious conflict of interest.
Thus the fact that this article has a strong bias towards presenting ME/CFS as an biopsychosocial condition (a bias which is not supported by any science) suggests that some of the main editors here who are promoting the biopsychosocial view may be paid stooges for the disability insurance industry. So can people like Doc James, sciencewatcher and others here who have a pro-biopsychosocial stance categorically state that they are not being paid by the disability insurance industry, and are not receiving any form of benefit from this or any other industry or outside interests? There are several people who are persistent editors on this ME/CFS page, who work hard and tirelessly to make ME/CFS look as if it were a biopsychosocial illness.
Wikipedia does have many editors who are paid by corporate interests to manipulate articles; see here for example: Some People Get Paid a Lot of Money to Edit Wikipedia Pages. Wikipedia rules state that paid editors who receive compensation for their contributions to Wikipedia, either directly or indirectly, MUST disclose who is paying them to edit. So that is why I am asking the editors of this page who have a pro-biopsychosocial view of ME/CFS and a major interest in this article to declare whether or not they receive any form of payment, benefit or compensation for their work on this article. — Preceding unsigned comment added by 46.208.234.40 (talk) 01:49, 17 November 2017 (UTC)
- @46.208.234.40 Er uh humm.... Don't think Doc James,is paid by the disability insurance industry in anyway or form. He appears to come across as a very genuine and knowable medic (which takes many years of study and hands-on-experience to get to that level of expertise). Problem is that on CFS he often appears comes across as a shoemaker that doesn't keep to his last and pontificates in area which he has little understanding. Think this is the real issue... For being an expert in one range of areas doesn't qualify one to be and expert in everything. As for Sciencewatcher, she comes across as only interested in the it is all in the mind explanations. In the past, this view was very popular – but has fallen (by much earlier than present 2017) to the wayside of wishful thinking without any science coming forth to back it up. Therefore, we should not pay these brief bright, brilliant and flash-in-the-pan ideas any credence no more. We need (as you sense) to keep moving this article on - in order to keep it current encyclopedic. Aspro (talk) 16:59, 18 November 2017 (UTC)
- Aspro, if you put as much effort into improving the article as you do writing your weird psychological rants, it might improve the article. I'm not sure how you conclude that I think CFS is imaginary when I add info on XNRV, hormomes, immune system, etc. Perhaps because I revert edits from people like you who keep removing psychological studies that are supported by evidence? The thing is, if you really want to be a useful wikipedia editor you have to edit based on the references available, rather than your personal opinions of the science. I also find it amusing that you can't bother to look at my user page to see my gender. Also amusing that I've been accused of being in the pocket of the HFCS, MSG, electricity, and pharma (anti GcMAF) companies, and now the insurance companies! I guess if you edit a controversial article and haven't been accused of some conspiracy theory, you're probably doing something wrong.
- It would be useful for everyone to have another look at WP:CAN. The reason we've suddenly got this rash of lunatic fringe conspiracy theorists is due to a round of canvassing on Phoenix Rising. --sciencewatcher (talk) 22:59, 18 November 2017 (UTC)
- sciencewatcher, you have not yet answered the question of whether you receive money or any other form of benefit for your work on this article. And neither so far has Doc James; he says on his user page that he does not receive money for his work on Wikipedia, but there are other non-pecuniary ways to receive benefit. So a clear statement would be appreciated.
- And by the way, if you are that naive to think that biopsychosocial notions of disease are all pure and genuine science, and have been oblivious to the fact that biopsychosocial departments in universities have been funded and paid for by the disability insurance industry (details of which I can provide on request) in order to try to make expensive-to-support organic diseases look as if they are partially psychogenic (which as explained earlier saves insurance companies billions), then one wonders whether you should be engaging in such responsible work as Wikipedia Medical editing. Of course the Internet is abound with innumerable crackpot conspiracy theories, and the innumerable halfwits who subscribe to them. However, that's no excuse for naivety about the way corporate agendas can and do manipulate science, as well as influence government policy.
- But it's not clear whether you are just a little naive, or whether you know full well how the disability insurance industry are promoting biopsychosocial ideas of disease, because you are receiving payment for such promotion. That's why a clear statement from you and others here regarding whether you receive compensation or other forms of benefit for your work on this article would help clear things up. — Preceding unsigned comment added by 46.208.234.40 (talk) 02:03, 19 November 2017 (UTC)
- Actually, Doc James and I are both chemtrails pilots, and we get paid very well for keeping the population in check. In our spare time we get paid by the HFCS, MSG, electricity, wifi and insurance industries to edit the wikipedia articles to prevent the truth getting out. CFS is actually caused by the government putting drugs into the water supply of people who come too close to figuring out the truth. The insurance industry is happy to pay millions of pounds to patients rather than them know the truth. Paying us to edit wikipedia, and paying Cochrane to publish fake research is a good cover story. --sciencewatcher (talk) 16:39, 19 November 2017 (UTC)
{kind=link}
- sciencewatcher you have for a second time refused to answer the question regarding any conflicts of interest you may have in relation to this article. If you have no such COIs, it would be easy for you to make a categorical statement here that you have never received any payments or other benefits for your work on this article, or have any other conflicts of interest that may prejudice your editing of this article. Yet in spite of being asked twice, you have not made such a statement, even though wikipedia guidelines state that conflict of interest issues should be addressed in the first instance on article talk pages.
- So for a third time, this is a request for your conflict of interest statement. If you do not provide one, it can only be assumed that you do have conflicts of interest, and thus the appropriate course of action would be to report you on the Wikipedia Conflict of interest Noticeboard.
- I have alerted Doc James to this discussion via his user page, because a categorical statement indicating that he has no conflicts of interests would also be appreciated.
- You may wish to read Wikipedia's guidelines on conflicts of interest. In particular, note the definition of a COI: "Any external relationship—personal, religious, political, academic, financial (including holding a cryptocurrency), or legal—can trigger a COI."
- I haven't answered because you're being a dick in asking this in the first place. There's no evidence of any COI from anyone here, other than your delusional accusations, which I'm quite happy to fuel for my own amusement. --sciencewatcher (talk) 21:18, 19 November 2017 (UTC)
With respect to COI, I make no money from editing Wikipedia in any way shape or form and never have. I do not work for an insurance company and never have. In fact I have donated a fair bit to the WMF over the years (more than $10,000) and as I personally only publish open access have paid to publish the research I do on the topic. Doc James (talk · contribs · email) 22:30, 19 November 2017 (UTC)
- Thank you Doc James for your response, and for confirming that you have no disability insurance connections. Can we presume that you don't have any other conflict of interest areas, because it is not just financial COIs that are a concern in the Wikipedia's guidelines on COI: any external relationship has the potential to create to a COI.
- Chronic fatigue syndrome is a controversial area, therefore it is even more important than normal to ensure that editors who regularly work on this article have no conflicts of interest.
- sciencewatcher, with a bit of background checking, I managed to find a possible conflict of interest area that you have, namely a published academic study, a published book, and an website which all clearly advocate the psychogenic view of chronic fatigue syndrome, and indeed advocate the psychogenic view of several other diseases and conditions. I will not link to them here, in order to protect privacy. Thus the fact that you have something of a career in promoting the psychogenic view of ME/CFS and other diseases may be grounds for a COI. I think raising this issue on the Wikipedia conflict of interest noticeboard may be appropriate, as it seems unlikely that you will be able to edit this article with the necessary neutrality if, externally to Wikipedia, you are championing the psychogenic view of ME/CFS. The heart of the controversy about ME/CFS are the two competing views of the aetiology this disease: the view that ME/CFS is a psychogenic "all in the mind" condition versus the view that ME/CFS is a biologically-caused organic diseases. Your external career as an advocate and a promotor of the psychogenic view would appear to introduce a COI, and make you an unsuitable editor of this article. — Preceding unsigned comment added by 46.208.234.40 (talk) 02:11, 20 November 2017 (UTC)
- Nope, that's all bullshit. I don't have any "career" in CFS, or make any money whatsoever from it. I'd suggest you stop this wasting our time, avoid making baseless accusations, and be civil. This kind of shit may be fine on Phoenix Rising, but you should be aware that it isn't tolerated here. --sciencewatcher (talk) 02:23, 20 November 2017 (UTC)
- Also, it seems you don't understand what COI actually is. Even if I was selling a book about CFS (which I'm not), that wouldn't be a COI unless I promoted my book here. --sciencewatcher (talk) 02:29, 20 November 2017 (UTC)
- Civility would be courteously replying to a perfectly reasonable request for a conflict of interest statement from you, which you flatly refused to do, preferring instead to respond to the request in a facetious and cagey manner. Your cageyness regarding COI issues is inexplicable — unless of course you have hidden COIs. In addition to refusing to answer on COI issues, you now appear to be blatantly lying: you say you are not selling a book, but your book about your psychogenic theories of ME/CFS and other diseases is available to buy on Amazon. From your book it is clear that you are an advocate and promotor of you own personal psychogenic view of chronic fatigue syndrome and other diseases, and that you are financially profiting from this promotion. So I think Wikipedia COIN needs to look into your circumstances, and I will be opening a COIN case shortly.
- Please do not remove my text again. It is not a personal attack; it is simply fact that you are lying when you say you are not selling a book about your psychogenic theories of ME/CFS. I am not sure what you think you will gain by lying, as I am going to provide COIN with a link to your book that is available on Amazon, so the evidence for the existence of your book is incontrovertible. 46.208.234.40 (talk) 14:13, 21 November 2017 (UTC)
- The case of sciencewatcher's potential COI has now been raised on the Conflict of interest Noticeboard. This COIN case is entitled:
- "Chronic fatigue syndrome article — longstanding editor Sciencewatcher has a potential COI".
- (For future reference, the diff link to the COIN case is here. 46.208.234.40 (talk) 15:30, 21 November 2017 (UTC)
- Note that that "discussion" has been closed. -Roxy, Zalophus californianus. barcus 08:20, 22 November 2017 (UTC)
- (For future reference, the diff link to the COIN case is here. 46.208.234.40 (talk) 15:30, 21 November 2017 (UTC)
- Yes I have no COIs with respect to this topic. Doc James (talk · contribs · email) 15:51, 21 November 2017 (UTC)
- ^ "Chronic fatigue syndrome: a review". PMID 12562565.
{{cite journal}}: Cite journal requires|journal=(help) - ^ "Risk factors for chronic fatigue syndrome/myalgic encephalomyelitis: a systematic scoping review of multiple predictor studies". PMID 17892624.
{{cite journal}}: Cite journal requires|journal=(help) - ^ "Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness". PMID 25695122.
{{cite journal}}: Cite journal requires|journal=(help) - ^ Cite error: The named reference
Smith2015was invoked but never defined (see the help page). - ^ a b Cite error: The named reference
Lil2016was invoked but never defined (see the help page). - ^ http://journals.sagepub.com/toc/hpqa/22/9
- ^ http://www.npr.org/sections/health-shots/2017/10/02/554369327/for-people-with-chronic-fatigue-syndrome-more-exercise-isnt-better
- ^ https://www.statnews.com/2017/09/25/chronic-fatigue-syndrome-cdc/
- ^ https://www.ncbi.nlm.nih.gov/pubmed/23480562
- ^ International Classification of Diseases. I. World Health Organization. 1969. pp. 158, (vol 2, pp. 173)
- ^ http://www.name-us.org/DefintionsPages/DefinitionsArticles/Hoopersdescription.pdf
Brain inflammation in ME/CFS
Guy, I am posting this here, because there is something wrong with your user talk page that does not allow editing.
You said on the Conflict of interest Noticeboard (COIN) page that:
"Insistence on the term "myalgic encephalomyelitis" automatically marks you out as one of the warring parties"
Where did you get that idea? In fact I usually call it "chronic fatigue syndrome", as it is easier to pronounce. I put both ME and CFS for clarity when writing the COIN case, and because they are often used interchangeably. But actually, ME is the more correct term, as the disease ME is listed in the World Health Organization ICD-10, whereas CFS is not listed (CFS is only found in the American localization of the ICD-10).
"I am not aware of any evidence that this is objectively proven to be a form of encephalomyelitis (feel free to fill a gap in my knowledge there)"
So I take it you have not seen this study: Neuroinflammation in Patients with Chronic Fatigue Syndrome/Myalgic Encephalomyelitis: An ¹¹C-(R)-PK11195 PET Study
- One primary source, small number of patients, and no reference to myelin. They may be onto something, in which case the name will probably not be encephalomyelitis, as far as I can see. Guy (Help!) 10:54, 22 November 2017 (UTC)
"a minority, for whom the mere suggestion that the condition has any psychological component whatsoever is utterly unacceptable, to the point that they will attack anybody who even thinks about trying CBT as part of palliative treatment. I trust you are not one of those people"
The issue is that many doctors in the UK, the US and elsewhere only see ME/CFS as a psychologically-caused condition, and will thus often refuse to give you antivirals, which several published studies have shown to be of benefit for ME/CFS (not surprising given ME/CFS usually starts after a viral infection). In the UK, doctors are not allowed to prescribe antivirals for ME/CFS, presumably because many in the NHS and GMC see ME/CFS as a psychologically-caused condition. Nobody would mind if ME/CFS was seen as a primarily organic physically-caused disease, which may in some cases have a minor psychological component. But medical services often see ME/CFS as only a psychological-caused condition, and refuse to treat it as an organic disease. This article only serves to reinforce the psychogenic bias, with its focus on (largely ineffective) psychological interventions, rather than interventions that address the physical basis of the disease (such as antiviral treatment).
- I find this contentious. Wherever I have had any contact with medical professionals working on CFS, they have never supported this purported psychology-only view. Equally, they don't see it as primarily physical, they see it as a condition of unknown cause. Which is absolutely correct. Guy (Help!) 10:54, 22 November 2017 (UTC)
"The use of pejoratives like "all in the mind" and "psychogenic" is profoundly unhelpful"
Psychogenic is not a pejorative term! Psychogenic simply means "psychologically-caused, rather than physically-caused". If you feel very depressed because your girlfriend left you, that is a psychologically-caused (psychogenic) depression. If you feel depressed because a neurological disease is affecting your brain functioning, that is a physically-caused depression. "All in the mind" is just a quick way of explaining what psychogenic means.
- It is unhelpful in context. It portrays this as a battle between two opposite extremes, whereas the consensus view is neither. Guy (Help!) 10:54, 22 November 2017 (UTC)
" I've had PTSD, I have experienced this first hand"
Sorry to hear that. PTSD does however often appear to be a much more psychogenic condition, arising from extreme psychological stress, and thus possibly more amenable to CBT. Although it's interesting that recent evidence has shown that on the battlefield, PTSD appears to be linked to the brain damage caused by the shockwave of explosions (even though you may be far enough away from the explosion not to receive any overt physical injuries, the explosion's shockwave (a type of non-linear sound wave) is now known to cause subtle damage to the brain). Shell shock may have been caused by the same shockwave mechanism. 46.208.234.40 (talk) 00:14, 22 November 2017 (UTC)
- Head trauma was involved. Guy (Help!) 10:54, 22 November 2017 (UTC)
- It's of interest that head trauma can cause three different ME/CFS-like conditions: post-concussion syndrome, hypopituitarism (which occurs in up to 30% of moderate or severe traumatic brain injury) and syringomyelia (if a there is a trauma to the spine). Plus some studies suggest a neck injury can trigger fibromyalgia, and even ME/CFS has been known to appear after a physical trauma such as a road accident. 46.208.234.40 (talk) 15:26, 22 November 2017 (UTC)
- Even with PCS caused by physical trauma, psychological factors appear to be important and psychotherapy has been shown to help. The mind is in the brain, after all...there is no weird cartesian dualism going on. It's only tangentially related to this article though. --sciencewatcher (talk) 16:12, 22 November 2017 (UTC)
- Psychological factors are certainly important in keeping psychiatrists in work: many psychiatrists know so little about biochemistry, immunology, neurology, etc that they would never be able to work in any hard science branch of medicine; they are only fit for the soft science of psychology. Psychiatrists often spent their entire careers looking at the mind, and forgetting that the mind is underpinned by the physical organ of the brain. They live and breathe their little world of mind, but are too parochial to see a bigger picture that includes the biological underpinnings of mind. This kind of incompetence and narrowness of perspective needs to be called out. Their profession is long overdue for major overhaul, in order to make it properly scientific.
- Because of their short-sighted narrow outlook, when psychiatrists find that mental conditions are statistically a risk factor for physical diseases like say ME/CFS, they invariably assume that the mental symptom itself causes the increased risk. But this assumption just reflects their limited intellectual skills, because they often fail to appreciate that a mental symptom can be caused by physical abnormalities in the brain, and it may be those underlying physical abnormalities in the brain, not the mental symptom that arises from them, that creates the increased risk. Do you understand the difference between causality at the level of mind, and causality at the level of brain? Many psychiatrists don't; they only know about the former, and are not broad enough to understand and incorporate the latter. That may be for historical reasons: during the development of psychology in the 20th century, there was relatively little knowledge about the brain, so psychiatrists could only focus on mind; but in recent decades we've learnt a huge amount about the brain and the body, but psychiatrists are still wallowing in an out-of-date 20th century mind-only perspective.
- A new breed of psychiatrists is needed that don't just have empathetic skills that can probe the mind, but also have the sort of intelligence that will enable them to understand biology and the brain, so that they can begin to explore how mental symptoms may have physical causes. Even Prof Peter White, author of the flawed PACE CBT/GET trial, who is much disliked by ME/CFS patients for various reasons, must be given credit for stating that in mental health, increasing evidence points to mental illness being due to underlying physical disfunction of the brain, rather than due to mental causes (psychogenic factors). For example, new studies are showing that immune system-driven neuroinflammation is found in various mental health conditions such as depression, bipolar, schizophrenia and OCD. So there is hope that in future psychiatrists become a little less parochial, and will learn a bit more about biology. 46.208.234.40 (talk) 18:53, 22 November 2017 (UTC)
- ^^^^This off topic stuff has little or nothing to do with improving the article. -Roxy, Zalophus californianus. barcus 18:59, 22 November 2017 (UTC)
- A new breed of psychiatrists is needed that don't just have empathetic skills that can probe the mind, but also have the sort of intelligence that will enable them to understand biology and the brain, so that they can begin to explore how mental symptoms may have physical causes. Even Prof Peter White, author of the flawed PACE CBT/GET trial, who is much disliked by ME/CFS patients for various reasons, must be given credit for stating that in mental health, increasing evidence points to mental illness being due to underlying physical disfunction of the brain, rather than due to mental causes (psychogenic factors). For example, new studies are showing that immune system-driven neuroinflammation is found in various mental health conditions such as depression, bipolar, schizophrenia and OCD. So there is hope that in future psychiatrists become a little less parochial, and will learn a bit more about biology. 46.208.234.40 (talk) 18:53, 22 November 2017 (UTC)
- How do you know that? Such discussions might led to a major shift in intellectual perspective in some of the editors here, resulting in fundamental changes to the article. 46.208.234.40 (talk) 19:09, 22 November 2017 (UTC)
- It seems unlikely that a discussion here would significantly affect anyone's outlook, and it's still against wikipedia talk page policies. Anyway, I don't think any of the long-time editors here are the problem...we all adhere to WP:MEDRS and WP:WEIGHT. I'm pretty sure all of us here already know that both psychological and organic causes are known to trigger the release of inflammatory cytokines and depression/anxiety (if not, it's probably worth reading up on it). You seem to want us to remove studies from the page that you don't personally agree with, which is never going to happen. If there are any specific problems with the page, feel free to bring them up here. --sciencewatcher (talk) 19:48, 22 November 2017 (UTC)
- You deleted my comment again. Touchy.
- The particular details of which studies are or are not included in the CFS article I am not concerned with. What I am concerned with is that there is no more evidence ME/CFS is psychogenic than multiple sclerosis is psychogenic. The Wikipedia multiple sclerosis article does not suggest that psychogenic factors are involved in MS, thus neither should the CFS article. CBT and exercise are used in MS, but the MS article only mentions these in passing, in just once sentence. The CFS article should do likewise: at most it should mention exercise and CBT just in passing, in no more than a sentence or two. But really the CFS article should not mention exercise therapy and CBT at all, because these are not to be found in the CDC treatment guide for CFS. The only mention of exercise should be in the context of post-exertional malaise (PEM), explaining that physical exertion (and sometimes mental exertion) can trigger PEM.
- Far too many people (the general public and doctors alike) already erroneously think that ME/CFS is an "all in the mind" condition, such that they then blame the patient for their illness, when there is no real evidence for such a psychogenic aetiology. The Wikipedia CFS article as it stands, with its focus on psychogenic factors and psychological treatments, only serves to reinforce this erroneous idea that ME/CFS is "all in the mind", which reinforces the idea that ME/CFS patients are to be blamed for their own condition, reinforces the idea that ME/CFS patients are not worthy of medical help, and reinforces the idea ME/CFS is not worth spending any research dollars on. ME/CFS patients already face these problems, and the Wikipedia article as it stands only serves to fortify these erroneous prejudices. 46.208.234.40 (talk) 23:30, 22 November 2017 (UTC)
The quoted comments from Guy are a worrying example of the sorts of prejudices which seem to have been institutionalised within wikipedia's coverage of CFS. I realise wikipedia's policies discourage people from doing 'original research', or seemingly any sort of independent thinking, but this is surely going too far. Check this discussion between Wessely and Shorter for 'all in the mind' if you do not know of anyone who would promote such a view of CFS: www.sjweh.fi/download.php?abstract_id=252&file_nro=1 That view of the controversies surrounding the labelling of patient's symptoms seems entirely founded on one-sided propaganda (if you do not mention the legal implications of differing labels for financial matters, you are not making an informed comment, and given the role of researchers reporting insurance industry COIs in this area, this has wider implications).
Even as international academics are praising patients for pointing out serious problems with the work claiming to indicate the efficacy of CBT as a treatment for ME/CFS, you continue to promote the stigmatising portrayal of unnamed bogeymen "for whom the mere suggestion that the condition has any psychological component whatsoever is utterly unacceptable, to the point that they will attack anybody who even thinks about trying CBT as part of palliative treatment"? Peter Tatchell commented on twitter that "Stigmatising ME/CFS #PACEtrial critics reminds me of reaction when I opposed aversion therapy for gays in 1972". I think that editors here need to think very seriously about their own moral responsibilities, and what they would have to do to make amends for promoting junk-science of prejudices from authority figures. If you were editing wikipedia at a time when authority figures were still claiming that nonblinded trials relying on subjective self-report outcomes were a legitimate justification for claiming homosexuality could be 'treated' by aversion therapy, would you have a duty to think critically about their claims? Or their attempts to claim that those gay rights campaigners who challenged them were engaging in a campaign of anti-science harassment? I fear that many here would still think that it would be best to defer to the prejudices of those with power in society, however maybe a few will realise that this is not a morally respectable way to behave.
Badly biased in some parts...
Article is a mix of quite good and some really bad(and apologies in advance for not providing links, but it would take me hours to find them again(and the couple of links i do have are not in English))...
-
The article relies far too much on the faked results and what that resulted in from the PACE study(which has already been thoroughly debunked, and might even lead to courtroom action against the responsible people), where the involved people faked positive results by altering the definitions of "sick"(objectively, people got WORSE from GET, yet the official presentation claimed they got better). No, extremely much NO, "cognitive behavioral therapy and a gradual increase in activity" does NOT have any valid evidence for positive effects.
-
Exercise therapy has in fact very clear evidence of NEGATIVE effects, while CBT at best just helps with mental issues caused by being sick. The only supposed evidence for that comes from the PACE excuse of a "study" and from when poor definitions are being used, mixing in patients that does not suffer from ICC G93.3(ME/CFS) but rather psychologically based issues like ICC F48 or in some cases even worse, people with PTSD, tiredness caused by stress or "burnout".
-
Also, there has been a number of symptoms found that so far have been very reliable, but with the problem that all of them can only be done in laboratory conditions or are very expensive, so no common testing is done.
Audio/visual distortions where the view/sound is interfered with between eye/ear and where actively perceived. This was also noted as a possible future way of diagnosing due to being apparently unique in how it affected patients(if they could find a way to measure it correctly with regular EEG).
Reduced functionality in mitochondria.
Reduced "circulating amount of blood", all the way from not possible to determine, to around 40% less than expected for a patient.
Fever in the brain and/or brainstem, despite overall body temperature being normal or even below normal. The researchers in this case had to develop a brand new way of measuring temperature from bloodchemistry to get a result.
There is a genetic sequence that clearly increases the risk of contracting ME/CFS, but none has been found to be the cause.
Detailed studies researching causes found that over 90% of patients had their ME/CFS begin after an infection(any kind, but with less than 10 responsible for over 80% of patients), and those where such was not found, the diagnosis was uncertain, giving strong support to suggestions that ME/CFS is caused by infection.
Patients aerobic and anaerobic energy systems function poorly, while the system that provides energy for the initial momentary action is not or much less affected.
-
Also, no mention at all was made about the Rituximab clinical trials ongoing in Norway, after a cancer specialist found that a majority of his patients with ME/CFS improved greatly after treatment with the immunomodulating substance(it destroys B-cells).
-
Very importantly, the Fukuda definitions IS NOT the generally accepted one! The Canada criteria is. And the most recent, the SEID criteria isn't even mentioned! Despite possibly/probably being the most correct one.
DW75 (talk) 16:43, 21 November 2017 (UTC)
- Interesting speculation. -Roxy, Zalophus californianus. barcus 17:03, 21 November 2017 (UTC)
- Well, as it happens just hours after writing the above, i ran into some relevant news on the subject:
- https://www.omf.ngo/2017/11/15/sgtc-research-conference-includes-focus-on-mecfs/
- Especially interesting is the part mentioned about biomarkers "2) 21 cytokines are different between ME/CFS patients and controls; 3) 27 clinical tests are different between patients and controls, including low morning cortisol in patients; 4) 63 metabolites are different between patients and controls"
- And no, nothing of what i wrote was speculation, it's just hellishly troublesome to find the correct links to reference everything, as pretty much every part of what i wrote comes from different sources, and most of what i have saved is in my own language and as such not really suitable for the English wikipedia. I did find one more link buried in my saved links, this is essentially the final nail in the coffin of the PACE study:
- http://journals.sagepub.com/toc/hpqa/22/9
- Well, as it happens just hours after writing the above, i ran into some relevant news on the subject:
DW75 (talk) 19:23, 21 November 2017 (UTC)
Unfortunately the results of the phase III trials of Rituximab were negative. C7762 (talk) 08:43, 22 November 2017 (UTC)
User:DW75 Any changes need to be referenced by WP:MEDRS sources, so it can be difficult to get changes made. Having said that there are 2 recent sources that you may find helpful. 1. https://www.cdc.gov/me-cfs/index.html which was discussed at Talk:Chronic_fatigue_syndrome/Archive_19#The_CDC_guide_has_been_updated. where my suggestions were rejected in part because https://www.cdc.gov/features/chronic-fatigue-syndrome/index.htm still pointed to the old version. But this has now been updated redirects to https://www.cdc.gov/features/cfsawarenessday/. So the source needs revisiting. 2. The BMJ Best Practices was updated in July 2017 and may be of use. http://bestpractice.bmj.com/best-practice/monograph/277.html. full version:- https://drive.google.com/file/d/0B57eLIp17Q8MNEtlV2RnSG54N28/view
I would suggest changes related to Post exertional maliase would be a good starting point.The CDC guidance states PEM is now a core symptom and the BMJ guidance describes PEM in detail.
It is worth reading the last 2 or 3 archive pages of this talk page to get a feel of how hard it is to get changes made. C7762 (talk) 14:03, 23 November 2017 (UTC)
Archiving query
collapse per WP:TPG
|
|---|
|
Why has this been archived? It says at the top of this page that "This talk page is automatically archived by MiszaBot I. Threads with no replies in 3 weeks may be automatically moved." So why was my section archived prematurely? My section was meant to get the attention of any editors of this article, so it needs to remain here for some time. I also think it is particularly important that other editors see that you have some potential conflicts of interest, Sciencewatcher, so that when they work with you, they will know that you are a strong advocate of the psychogenic view of ME/CFS. Please return this archived section to this talk page. 46.208.234.40 (talk) 23:30, 22 November 2017 (UTC)
|
PVFS
It might be worth adding a section on PVFS, citing reviews which look at post-infectious CFS, and discussing PVFS vs CFS. Two recent (2010-) reviews are Hulme 2016, and Moss-Morris 2010. --sciencewatcher (talk) 02:43, 29 November 2017 (UTC)
- PVFS redirects back to this article so it seems relevant.Ward20 (talk) 04:23, 29 November 2017 (UTC)
- Yup Doc James (talk · contribs · email) 18:10, 29 November 2017 (UTC)
- I've made a stab at adding this info. The Hulme review isn't ideal (no citations as far as I can see) but is the only one I found that reviews precipitating factors. --sciencewatcher (talk) 23:12, 29 November 2017 (UTC)
Pace Trial
Should there be a section that talks about the pace trial? both the trial itself and the criticism? I found two sources here, primary sources that are from researchers calling for a retraction in one case, and a reevaluation of the data in another case. Not going to add yet as I am a new editor, but it seems like it could be valuable: http://www.virology.ws/2017/03/13/an-open-letter-to-psychological-medicine-about-recovery-and-the-pace-trial/ http://www.virology.ws/2015/11/13/an-open-letter-to-dr-richard-horton-and-the-lancet/ Gillesdeleuze13 (talk) 18:59, 15 January 2018 (UTC)
- The Pace trial is covered in more depth at Chronic fatigue syndrome treatment. Ward20 (talk) 00:21, 16 January 2018 (UTC)
Q-fever is bacterial
Under the heading "Viral Infection", Q-fever is listed as a risk factor. This requires editing, because Q-fever is bacterial in origin. Keyser42soze (talk) 15:40, 15 January 2018 (UTC)
- This section is fairly new and probably could use some more work. Good secondary WP:MEDRS sources need to be found for this. Ward20 (talk) 00:25, 16 January 2018 (UTC)
Ref needed
For this Doc James (talk · contribs · email) 12:42, 10 February 2018 (UTC)
Unrest movie
Unrest is a 2017 documentary by Jennifer Brea telling the story of her battle with chronic fatigue syndrome. Jennifer developed CFS shortly before her wedding, and was eventually bed-ridden with an illness that doctors told her was "all in her head". The movie was well received, and was shortlisted for an Academy Award nomination for Best Documentary Feature.
- Lots of refs in the "see also" link (didn't think it was really necessary for a short sentence about a Movie we have an article about, but should be easy to add). --sciencewatcher (talk) 16:12, 10 February 2018 (UTC)
- I agree needs a sentence or two with link to its own article (Wikipedia is after all a hypertext system) The above suggested edit looks good.C7762 (talk) —Preceding undated comment added 12:55, 25 February 2018 (UTC)
Autoimmunity
I tried previously editing the following sentence: "Autoimmunity has been proposed to be a factor in CFS; however, the only relevant finding is a subset of patients with increased B Cell activity and autoantibodies, possibly as a result of decreased NK cell regulation or viral mimicry." This is no longer true as there are now several autoantibody studies related to cholinergic receptors. Does anyone have suggestions re: how to reframe this in a way that would pass editorial muster so my edits don't get reversed? At the very least it should mention WHICH autoantibodies are repeatedly being found as the present sentence is generic. The new studies also don't mention it's only in a subset of those with increased B Cell activity (as far as I can see). Thanks!
References: https://www.ncbi.nlm.nih.gov/pubmed/12851722 https://www.ncbi.nlm.nih.gov/pubmed/29543914 https://www.ncbi.nlm.nih.gov/pubmed/26399744 http://journals.sagepub.com/doi/abs/10.4137/III.S25105 — Preceding unsigned comment added by Amy2890 (talk • contribs) 21:57, 18 March 2018 (UTC)
Research on causes - thyroid ?
Could Chronic Fatigue Syndrome Be a Thyroid Hormone Deficiency? could be mentioned (as a hypothesis) in Causes or Research ? - Rod57 (talk) 12:17, 26 March 2018 (UTC)
- It it were mentioned in a WP:MEDRS maybe. Alexbrn (talk) 12:33, 26 March 2018 (UTC)
Updating for the International Consensus Criteria
I noticed that this article references a 2003 CDC document as the "most commonly used diagnostic criteria." Further down, it references the Fukuda definition and the 2003 Canadian definition. However, there's no reference to the 2011 International Consensus Criteria. As far as I know, this is the current best definition, and nobody today is arguing that earlier descriptions are superior. However, I'm not an expert.
I suggest replacing much of the article's content (especially in the "signs and symptoms" and "diagnosis" section) with information from the International Consensus Criteria, instead of just adding more conflicting info. But that would be a pretty major change. Are there any objections?
Jfsupeene (talk) 21:43, 19 April 2018 (UTC)
The IOM Definition (2015)
The updates are good. The only suggestion I have is that the paragraph seems too long. That section in the CFS article is meant to just be a summary of the main clinical descriptions of CFS article, but your new summary paragraph is about the same length as the one in the clinical descriptions article. It should probably be about the same length as the other definitions. --sciencewatcher (talk) 03:22, 21 April 2018 (UTC)
ME/CFS or CFS/ME?
The name of the article needs discussion. Most all the new publications and the US and UK health organizations now refer to the name as Myalgic encephalomyelitis/Chronic fatigue syndrome or Chronic fatigue syndrome/Myalgic encephalomyelitis. The article needs to be updated to reflect the current naming conventions. Ward20 (talk) 06:31, 23 April 2018 (UTC)
- imho neither. It should not be called ME as no myelitis has been demonstrated. -Roxy, the dog. barcus 13:09, 23 April 2018 (UTC)
- ME is a well-accepted name for the condition, and a plurality- even majority- of medical experts are at least comfortable with calling it ME, even if that's not their preferred nomenclature. Wikipedia should reflect that, regardless of your personal opinion on the evidence. If the OP is right that the naming convention is shifting to ME/CFS (I've seen that used a lot too), then I'd agree we should replace "CFS" with "ME/CFS" throughout the article, with an explanatory nod in the lede. Or CFS/ME, whichever's more common, but I find ME/CFS rolls of the tongue more easily.Jfsupeene (talk) 22:19, 24 April 2018 (UTC)
Disputed tag
Why is there a dispute tag but no discussion here about any disputes? --sciencewatcher (talk) 13:46, 13 May 2018 (UTC)
Exercise again
We had a RfC about this wording:
- "Evidence suggests that cognitive behavioral therapy and a gradual increase in activity suited to individual capacity can be beneficial in some cases"
This is not specifically about GET but about exercise generally.
The AHRQ in 2016 says "The results are consistent across trials with improvement in function, fatigue, and global improvement and provided moderate strength of evidence for improved function (4 trials, n=607) and global improvement (3 trials, n=539), low strength of evidence for reduced fatigue (4 trials, n=607) and decreased work impairment (1 trial, n=480), and insufficient evidence for improved quality of life (no trials) (Table 7). By excluding the three trials using the Oxford (Sharpe, 1991) case definition for inclusion, there would be insufficient evidence of the effectiveness of GET on any outcome (1 trial, n=49)."
Thus it also supports the prior wording. GET in 2016 after excluding those using the Oxford definition, had only been studied in one trial involving 49 people thus it is not at all surprising limited conclusions could be drawn. Doc James (talk · contribs · email) 08:38, 14 June 2018 (UTC)
- Doc James, when you say "GET in 2016 after excluding those using the Oxford definition, had only been studied in one trial involving 49 people thus it is not at all surprising limited conclusions could be drawn" that is in accordance with the position of the AHRQ, i.e. there is insufficient evidence for GET! This is precisely the point, and when it is made by a US Federal Agency it ought to be included in any Wikipedia article which has NPOV as a fundamental principle of editorial policy. I find it bizarre that you would want to suppress the AHRQ report. NPOV: "which means representing fairly, proportionately, and, as far as possible, without editorial bias, all of the significant views that have been published by reliable sources on a topic." https://en.wikipedia.org/wiki/Wikipedia:Neutral_point_of_view. Regarding using the term graded exercise therapy, that is what is being referred to in the references cited in support of its effectiveness: "Trials of rintatolimod, counseling therapies, and graded exercise therapy suggest benefit for some patients meeting case definitions for CFS..." http://annals.org/aim/article-abstract/2607809/cytokine-inhibition-patients-chronic-fatigue-syndrome-randomized-trial; "Most studies asked participants to exercise at home, between three and five times per week, with a target duration of 5 to 15 minutes per session using different means of incrementation." "Comparator interventions ... Adaptive Pacing Therapy" http://cochranelibrary-wiley.com/doi/10.1002/14651858.CD003200.pub7/full. Breachdyke (talk) 10:53, 15 June 2018 (UTC)
- @Doc James: (courtesy ping). Kleuske (talk) 10:59, 15 June 2018 (UTC)
- WP:MEDRS? Kleuske (talk) 11:00, 15 June 2018 (UTC)
Sure by it says "Four trials evaluated the effectiveness of GET compared with a control group (n=656) (Table 6, Figures 3 and 4). Of these, three used the Oxford (Sharpe, 1991) case definition (n=607)12, 30, 41 while one small trial used the CDC (Fukuda, 1994) case definition (n=49).42 The results are consistent across trials with improvement in function, fatigue, and global improvement and provided moderate strength of evidence for improved function (4 trials, n=607) and global improvement (3 trials, n=539), low strength of evidence for reduced fatigue (4 trials, n=607) and decreased work impairment (1 trial, n=480), and insufficient evidence for improved quality of life (no trials) (Table 7)." Why not highlight that bit? Doc James (talk · contribs · email) 19:39, 15 June 2018 (UTC)
I've not highlighted it because the AHRQ conclusions are premised on a rejection of the Oxford criteria (as also the NIH), which I make clear in the sentence I've added to the article. If you want to highlight here or elsewhere on Wikipedia, evidence for CBT and GET efficacy which utilises the Oxford criteria, you're free to do so. As it is, to edit out the citation of the AHRQ conclusion is editorially unjustified by NPOV, the AHRQ's position being significant and cited from a reliable source. Breachdyke (talk) 22:13, 16 June 2018 (UTC)
- @Breachdyke (talk), detailing why there are conficting statements about GET is too confusing to accomplish properly in the lead. The GET exceptions you put in the lead are detailed in the body under Chronic fatigue syndrome#Exercise therapy. The compromise wording in the lead, "a gradual increase in activity suited to individual capacity can be beneficial in some cases" is more appropriate because the Sharpe cohort does respond to GET while the other cohorts may not. This is referenced by the source you applied also. Ward20 (talk) 00:59, 17 June 2018 (UTC)
- Agree with User:Ward20. Doc James (talk · contribs · email) 15:53, 17 June 2018 (UTC)
I think there are a couple of problems with the article lead: (a) It says that treatment is merely symptomatic. Yet as far as I'm aware CBT and exercise therapy studies are based on the fear avoidance theory, which is held to describe the fundamental disease mechanism, and therefore CBT/GET/exercise therapy are not merely symptomatic treatments, making the article lead self-contradictory. (b) The article lead contains a moderate claim for the efficacy of CBT and GET/exercise therapy in ME/CFS. Yet even that moderate claim is disputed in the real world. It depends on, for example, the view taken of the merits (or lack thereof) of causal inference in psychological research (http://journals.sagepub.com/doi/full/10.1177/1745691613491271), and the Oxford criteria (https://www.ncbi.nlm.nih.gov/books/NBK379582/; https://www.tandfonline.com/doi/ref/10.1080/21641846.2017.1273863?scroll=top). Yet in the article lead there is no balancing statement whatsoever. Breachdyke (talk) 14:05, 19 June 2018 (UTC)
- The statement in question is supported by a 2017 Cochrane review.[21] This review states "Patients with CFS may generally benefit and feel less fatigued following exercise therapy, and no evidence suggests that exercise therapy may worsen outcomes." We paraphrase that. Doc James (talk · contribs · email) 14:45, 19 June 2018 (UTC)
- And the opening CDC source says "There is no cure or approved treatment for myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). However, some symptoms can be treated or managed" - which supports the text saying treatment is symptomatic. To say otherwise, we'd need sources. Alexbrn (talk) 14:46, 19 June 2018 (UTC)
- @Breachdyke (talk). a) CBT and GET has not been widely claimed to cure the fundamental disease mechanism for many years. They only moderately affect some symptoms, typical of symptomatic treatment, so there is no contradiction.
Even the much criticised PACE trial[22] does not claim that exercise therapy is based on avoidance theory.It is only a hypothesis along others. It certainly did not statistically restore activity to healthy control levels, nor did it affect many other ME/CFS symptoms. b) The lead wording, "a gradual increase in activity suited to individual capacity can be beneficial in some cases", was carefully chosen to be inclusive of exercise and pacing therapies, not just GET. Reviews that are highly critical of GET still state that careful exercise therapy can be beneficial to some patients.[23][24]. The caveats that the AHRQ discussed about studies using the Oxford criteria have long been in the Exercise section, where you would expect it to be.Ward20 (talk) 21:18, 19 June 2018 (UTC)- Yes. The problem is that a subset of patients categorically reject this, on the basis that they (falsely) believe it implies that CFS is psychosomatic. They insist that it is "myalgic encepahlomyelitis", but there is no clear evidence that it is, in fact, a form of encephalomyelitis, there is no actual consensus on the aetiology at all. Guy (Help!) 09:04, 20 June 2018 (UTC)
- The other issue is that just hearing the name myalgic encepahlomyelitis is accepted as a serious issue, Chronic fatigue syndrome isn't. [25][26] In fact, the 2018 ICD-10-CM has now separated CFS and ME coding making them mutually exclusive and equating ME to Post Viral Fatigue.[27][28] I thought this would cause some ruckus in the Journals but I haven't seen a single article on it. Ward20 (talk) 06:17, 21 June 2018 (UTC)
- Huh. That is unexpected! Guy (Help!) 08:36, 21 June 2018 (UTC)
- The other issue is that just hearing the name myalgic encepahlomyelitis is accepted as a serious issue, Chronic fatigue syndrome isn't. [25][26] In fact, the 2018 ICD-10-CM has now separated CFS and ME coding making them mutually exclusive and equating ME to Post Viral Fatigue.[27][28] I thought this would cause some ruckus in the Journals but I haven't seen a single article on it. Ward20 (talk) 06:17, 21 June 2018 (UTC)
- Yes. The problem is that a subset of patients categorically reject this, on the basis that they (falsely) believe it implies that CFS is psychosomatic. They insist that it is "myalgic encepahlomyelitis", but there is no clear evidence that it is, in fact, a form of encephalomyelitis, there is no actual consensus on the aetiology at all. Guy (Help!) 09:04, 20 June 2018 (UTC)
- @Breachdyke (talk). a) CBT and GET has not been widely claimed to cure the fundamental disease mechanism for many years. They only moderately affect some symptoms, typical of symptomatic treatment, so there is no contradiction.
- And the opening CDC source says "There is no cure or approved treatment for myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). However, some symptoms can be treated or managed" - which supports the text saying treatment is symptomatic. To say otherwise, we'd need sources. Alexbrn (talk) 14:46, 19 June 2018 (UTC)
- The statement in question is supported by a 2017 Cochrane review.[21] This review states "Patients with CFS may generally benefit and feel less fatigued following exercise therapy, and no evidence suggests that exercise therapy may worsen outcomes." We paraphrase that. Doc James (talk · contribs · email) 14:45, 19 June 2018 (UTC)
Ward20, "CBT and GET has not been widely claimed to cure the fundamental disease mechanism for many years"; the PACE trial (which is the largest study of its kind and has not been retracted) claimed that CBT and/or GET effected in some patients a "strict criterion of recovery" (https://www.thelancet.com/pdfs/journals/lancet/PIIS0140-6736(11)60172-4.pdf?code=lancet-site). It is difficult to see how such a claim could be reconciled to the notion that CBT and GET are not claimed to be capable of curing the fundamental disease mechanism. "Even the much criticised PACE trial[29] does not claim that exercise therapy is based on avoidance theory"; compare the study protocol, "CBT will be based on the illness model of fear avoidance ... GET will be based on the illness model of deconditioning and exercise intolerance" (https://bmcneurol.biomedcentral.com/articles/10.1186/1471-2377-7-6). If the PACE investigators did not think the deconditioning was the result of fear avoidance, then what did they think it was the result of? Also, "The caveats that the AHRQ discussed about studies using the Oxford criteria have long been in the Exercise section, where you would expect it to be." This does not release the article lead from NPOV. It still needs a balancing statement (a single sentence would suffice).Breachdyke (talk) 11:29, 20 June 2018 (UTC)
DocJames, the Cochrane review is mostly based on Oxford studies, so until that issue is noted in the article lead it remains selective and therefore biased. Re Cochrane on worsening outcomes, "GET was associated with higher numbers of reported adverse events compared with counseling therapies or controls. Harms were generally inadequately reported across trials." (https://www.ncbi.nlm.nih.gov/books/NBK379582/). It's also self-evident that questions of selection criteria and harm cannot be separated (I mean in any given study, just what is the disease that is being studied?). Another issue which no-one has replied to is the whole issue of causal inference in psychological research ((http://journals.sagepub.com/doi/full/10.1177/1745691613491271) - given the widespread limitations of study design, is there (for the most part) any rational basis for it?.Breachdyke (talk) 11:29, 20 June 2018 (UTC)
Guy, "there is no actual consensus on the aetiology at all"; The success or otherwise of particular treatments allows inferences of aetiology and that is one reason why presentation of evidence re treatments needs to carefully observe NPOV. Aetiology is hardly a trivial matter. Psychotherapy of all forms includes an appeal to the volition of its subjects – ultimately a person’s will is involved because a totally recalcitrant patient cannot be a subject at all. Therefore a patient who is psychosomatically ill can, ultimately, be blamed for a failure to improve physically. This is a key point in the controversy around ME/CFS: in psychosomatic illness blaming patients is potentially justifiable, but in physical illness (where mental factors are not causally significant) it is not. Breachdyke (talk) 11:27, 20 June 2018 (UTC)
- A lot of editorial musing here. We should instead just stick to what the decent sources say (as we are). Please learn to WP:INDENT posts as a matter of courtesy to others. Unless new sourcing can be produced which reveals that knowledge on this matter has shifted, I suggests the consensus is clear and we leave this topic with no change to the article, for now. Alexbrn (talk) 11:30, 20 June 2018 (UTC)
- Sure, I'm pretty new to editing on Wikipedia, but if everyone indents then couldn't you end up with an incredibly narrow column of text?!Breachdyke (talk) 13:52, 20 June 2018 (UTC)
- Along with evidence I've already cited, I note shift in a recent report by the Dutch Health Council: "Medical disability assessors ... should not regard a patient’s decision to forego CBT or GET as inadequate recovery behaviour" (https://www.gezondheidsraad.nl/en/task-and-procedure/areas-of-activity/optimale-gezondheidszorg/mecfs). Breachdyke (talk) 17:52, 20 June 2018 (UTC)
- @Breachdyke (talk) I want to apologise about saying The PACE study did not claim fear avoidance. I confused it with the 2017 Cochrane review that talked about a couple of hypotheses that they say are unproven. I have struck though my mistake above. I believe my other comments are accurate. From the Cochrane review, the fear avoidance hypothesis (they call it 'deconditioning model') is a 7-18 year old hypothesis they say is unproven. The Gijs Bleijenberg, Hans Knoop article that you referenced that stated "strict criterion of recovery", is only a letter. Medical articles here don't give weight to letters because of WP:MEDRS guidance, (not a reliable source for this). (b) The lead doesn't even mention GET so there is nothing to balance in the lead about GET. The wording about exercise in the lead is supported by 3 references, and one of them is the AHRQ review. Ward20 (talk) 04:12, 21 June 2018 (UTC)
- Thanks Ward20 and no worries. Remember that PACE has not been retracted, the principle investigators have repeatedly said they stand by it's claim of moderate efficacy of CBT and GET and hence moderate support for the fear avoidance hypothesis on which the study was conducted, and it remains the largest trial of its kind. Re Knoop, yes fair enough it is a letter, and therefore not relevant editorially, but I will point out that the PACE PIs have had ample opportunity to correct the letter and associated reports in the press but haven't done so. A disturbing omission on their part which is guaranteed to undermine patient trust. Breachdyke (talk) 11:28, 21 June 2018 (UTC)
- @Breachdyke (talk) Oops. Patient groups don't like CBT and GET was edited into the lead in the last week week or so. I am neural about the wording, but if there is consensus for it, it should go near the treatment wording in the lead and have a better source. Ward20 (talk) 04:39, 21 June 2018 (UTC)
- There is enough evidence to show that this is not 'science vs patients'. The scientific and clinical community is divided. Breachdyke (talk) 11:28, 21 June 2018 (UTC)
- The problem there is that it's the ME Association, which is a group that is fundamentally opposed to the name CFS and the leading proponent of the idea that any effect of CBT or exercise is tantamount to dismissing it as psychosomatic. Guy (Help!) 08:33, 21 June 2018 (UTC)
- Not so Guy - see in particular section F: http://www.meassociation.org.uk/about/management/#Cognitive%20behavioural. Breachdyke (talk) 11:28, 21 June 2018 (UTC)
- The name says all we need to know. Guy (Help!) 09:40, 22 June 2018 (UTC)
Can anyone point to a single trial of CBT and GET/incremental/increasing exercise therapy that is either blinded or uses an objective outcome measure(s) or both, and shows efficacy? Breachdyke (talk) 14:27, 21 June 2018 (UTC)
- This is WP:NOTAFORUM. In the absence of concrete suggestions for article improvement, I suggest this conversation be closed. Alexbrn (talk) 15:02, 21 June 2018 (UTC)
- I don't think I'm going to get a consensus here but I suggest following the sentence in the article lead re CBT and exercise therapy with: "However, opinion in the scientific community is divided. The Dutch Health Council recommend that a patient's decision to forego CBT or GET should not be seen as inadequate recovery behaviour, and in the United States the Agency for Healthcare and Research Quality found, after excluding studies based on the controversial Oxford diagnostic criteria, that there was only weak evidence for cognitive behaviour therapy and insufficient evidence for graded exercise therapy." (https://www.gezondheidsraad.nl/en/task-and-procedure/areas-of-activity/optimale-gezondheidszorg/mecfs; https://www.ncbi.nlm.nih.gov/books/NBK379582/). Breachdyke (talk) 16:20, 22 June 2018 (UTC)
- Nope. Too detailed and specific to regional practices for lead, and AHRQ already covered in article. DHC material might get consensus in body of Chronic fatigue syndrome treatment sub-article. Ward20 (talk) 17:24, 22 June 2018 (UTC)
- Ok well it looks like we'll be revisiting some of this for the body of the article. I'll have a look as time permits. I still think the article lead is unbalanced. The attempt to make it balanced by nuances in the wording re evidence for CBT and graded exercise is helpful but arguably insufficient. Breachdyke (talk) 18:10, 22 June 2018 (UTC)
- I want to make a couple of points. Earlier in the discussion this was claimed: "The Gijs Bleijenberg, Hans Knoop article that you referenced that stated "strict criterion of recovery", is only a letter. Medical articles here don't give weight to letters because of WP:MEDRS guidance, (not a reliable source for this)." The cited article was actually a commissioned commentary in the Lancet which had been reviewed by the PACE researchers prior to publication. I don't know why it was thought this was just a letter.
- For those referring to the Cochrane review of exercise therapy, it is worth reading the criticisms from Robert Courtney and others now included within the review. For example Courtney points out problems with outcome switching, and a failure to accurately describe the reviews own data within the text of the review. Courtney points out that the data shows that "all but one health indicator (i.e. fatigue, physical function, overall health, pain, quality of life, depression, and anxiety, but not sleep) demonstrated a non-significant outcome for pooled treatment effects at follow-up for exercise therapy versus passive control", but this is not made clear to readers in the text or abstract. There are also further problems identified with this review, and the research underpinning it, which mean that its purported findings are of questionable value. Is there good reason to mention any possible treatment in the introduction when the evidence for efficacy is so weak?Rainywednesday (talk) 15:23, 23 June 2018 (UTC)
- Please see WP:MEDASSESS. Letters, correspondence, and comments are not reliable sources. Disputing a source as unreliable means that higher impact factor reliable secondary sources can be shown to oppose the original findings. CDC has withdrawn their CBT and GET positions (but doesn't say not to use them) and AHRQ recommends that new studies are necessary without using the Oxford criteria. NHS, Cochrane, and othe guidelines recommend CBT and GET. Without a large body of studies or meta analysis published in Journals that have high impact factors to dispute the position, editors are required to follow a proponderance of the reliable sources.Ward20 (talk) 16:34, 23 June 2018 (UTC)
- Ok well it looks like we'll be revisiting some of this for the body of the article. I'll have a look as time permits. I still think the article lead is unbalanced. The attempt to make it balanced by nuances in the wording re evidence for CBT and graded exercise is helpful but arguably insufficient. Breachdyke (talk) 18:10, 22 June 2018 (UTC)
- Nope. Too detailed and specific to regional practices for lead, and AHRQ already covered in article. DHC material might get consensus in body of Chronic fatigue syndrome treatment sub-article. Ward20 (talk) 17:24, 22 June 2018 (UTC)
- Which letters are you referring to? The Lancet commentary you had earlier claimed was a letter is not a letter and I do not know why you thought it was. Robert Courtney's comments within the Cochrane review do not need to be cited, as they are merely explaining the review itself. Anyone who takes the time to read the review carefully will see for themselves that "all but one health indicator (i.e. fatigue, physical function, overall health, pain, quality of life, depression, and anxiety, but not sleep) demonstrated a non-significant outcome for pooled treatment effects at follow-up for exercise therapy versus passive control". I directed people towards Courtney's comments in case some editors had not taken the time to read the full review carefully for themselves and wanted an easy to understand summary, rather that to suggest that they be cited themselves. I don't know what you are responding to with your final sentence. Cochrane reviews are not guidelines, and NICE have recently decided that their guidelines for CFS need a full review. Anyway, I am not aware of either having stated that the evidence of efficacy for exercise therapy as a treatment of CFS is of such high quality that it should be referred to in the introduction of the CFS wikipedia article, and that is what I was questioning.Rainywednesday (talk) 16:52, 23 June 2018 (UTC)
Sorry, is this letter/not-letter piece PMID 21334060? If so, as a 7-year-old "comment" it is not WP:MEDRS. Alexbrn (talk) 17:31, 23 June 2018 (UTC)
- Yes, that's the piece. The Lancet commentary was cited above like this: "Ward20, "CBT and GET has not been widely claimed to cure the fundamental disease mechanism for many years"; the PACE trial (which is the largest study of its kind and has not been retracted) claimed that CBT and/or GET effected in some patients a "strict criterion of recovery" (https://www.thelancet.com/pdfs/journals/lancet/PIIS0140-6736(11)60172-4.pdf?code=lancet-site). It is difficult to see how such a claim could be reconciled to the notion that CBT and GET are not claimed to be capable of curing the fundamental disease mechanism." This was then responded to with this inaccurate claim: "The Gijs Bleijenberg, Hans Knoop article that you referenced that stated "strict criterion of recovery", is only a letter." I pointed out that it was not a letter just to prevent this misunderstanding from affecting peoples' judgements. I certainly don't think that it is a reliable source, but it is an example of misleading claims being made about the value of CBT and GET in high impact factor journals. What Bleijenberg and Knoop had described as a "strict criterion of recovery" relied only on subjective self-report outcomes from a non-blinded trial, and was so loose a criteria that patients could report declines from baseline on every outcome and yet still be classed as 'recovered'.Rainywednesday (talk) 17:42, 23 June 2018 (UTC)
- Ok I'll agree, it's a comment and not a letter, but still is fairly meaningless to providing evidence the fundamental hypothesis of GET is curing the fundamental disease mechanism (which I believe was the original argument of the editor, not me). Putting aside PACE for the moment and getting back on topic, the original objection was to the lead wording, "a gradual increase in activity suited to individual capacity can be beneficial in some cases." I haven't seen any sources disputing that. CDC has removed their recomendation of GET but states, "Patients who have learned to listen to their bodies might benefit from carefully increasing exercise to improve fitness and avoid deconditioning."[30] Ward20 (talk) 19:04, 23 June 2018 (UTC)
- I get the impression that the discussion about 'recovery' followed on from earlier, now archived, discussions, so I do not know if I really understand the context behind it, but if it was the case that CBT or GET led to 30% of patients fulfilling a genuinely strict criterion for recovery at 1 year follow up, then it would be reasonable to assume that these interventions were overcoming whatever if was that was causing the illness in some of these patients. While different people say different things, and CBT/GET researchers seem to be rapidly becoming much more modest in the claims they make for themselves and their treatments, there are many examples of them previously presenting CBT/GET as being designed to lead to full recovery. eg: The CBT manual that was cited as the basis for PACE's CBT states that: "The main goal of the treatment is full recovery, the supplementary objective being return to the workplace." CHAPTER 23 of the Handbook for CFS; 'Cognitive-Behavioral Therapies' Gijs Bleijenberg, Judith Prins, and Ellen Bazelmans.
- "Rainywednesday, "if it was the case that CBT or GET led to 30% of patients fulfilling a genuinely strict criterion for recovery at 1 year follow up, then it would be reasonable to assume that these interventions were overcoming whatever if was that was causing the illness in some of these patients." Agree entirely. This is the only reasonable assumption that could be made. Breachdyke (talk) 08:55, 26 June 2018 (UTC)
- Richard Horton seemed to view claims about recovery as central to the PACE trial, promoting its publication by explaining it like this: "Yeah, I mean adaptive pacing therapy essentially believes that chronic fatigue is an organic disease which is not reversible by changes in behaviour. Whereas cognitive behaviour therapy obviously believes that chronic fatigue is entirely reversible. And these two philosophies are kind of facing off against one another in the patient community and what these scientists were trying to do is to say, 'Well, let's see. Which one is right?'"
- re the introduction: There are many things that might benefit patients, but when the evidence for the efficacy of any particular treatment is so weak and contested, is there good reason to mention any of them in the introduction, where there will not be room to go into the details of the dispute and the reasons for ongoing uncertainty?Rainywednesday (talk) 03:06, 24 June 2018 (UTC)
- Agreed. At present the article lead contains an evidentially contestable statement, yet in the article lead it stands uncontested. NPOV is not being followed. Breachdyke (talk) 11:00, 26 June 2018 (UTC)
- I get the impression that the discussion about 'recovery' followed on from earlier, now archived, discussions, so I do not know if I really understand the context behind it, but if it was the case that CBT or GET led to 30% of patients fulfilling a genuinely strict criterion for recovery at 1 year follow up, then it would be reasonable to assume that these interventions were overcoming whatever if was that was causing the illness in some of these patients. While different people say different things, and CBT/GET researchers seem to be rapidly becoming much more modest in the claims they make for themselves and their treatments, there are many examples of them previously presenting CBT/GET as being designed to lead to full recovery. eg: The CBT manual that was cited as the basis for PACE's CBT states that: "The main goal of the treatment is full recovery, the supplementary objective being return to the workplace." CHAPTER 23 of the Handbook for CFS; 'Cognitive-Behavioral Therapies' Gijs Bleijenberg, Judith Prins, and Ellen Bazelmans.
- Ok I'll agree, it's a comment and not a letter, but still is fairly meaningless to providing evidence the fundamental hypothesis of GET is curing the fundamental disease mechanism (which I believe was the original argument of the editor, not me). Putting aside PACE for the moment and getting back on topic, the original objection was to the lead wording, "a gradual increase in activity suited to individual capacity can be beneficial in some cases." I haven't seen any sources disputing that. CDC has removed their recomendation of GET but states, "Patients who have learned to listen to their bodies might benefit from carefully increasing exercise to improve fitness and avoid deconditioning."[30] Ward20 (talk) 19:04, 23 June 2018 (UTC)
- re the introduction: Even though advocates for CBT and exercise therapy are now more circumspect, they are therapies statistically deemed beneficial in studies for the patient cohort treated and supported by high impact secondary WP:MEDRS sources NHS[31], AHRQ[32], and Cochran[33] as previously discussed here at talk. I know of no other therapies that can be sourced like that. Ward20 (talk) 04:49, 24 June 2018 (UTC)
- NHS is based on NICE, whose guideline on ME/CFS is moot because NICE say it needs a full review and that is now underway. AHRQ reject the Oxford criteria ("should be retired", "may impair progress and cause harm") and having done so find insufficient evidence for GET (the Cochrane review you cite - "a negotiated, incremental increase in the duration of time spent physically active followed by an increase in intensity", i.e. indistinguishable from "gradually increasing exercise suited to individual capacity..." in the article lead) and only weak evidence for CBT (https://www.ncbi.nlm.nih.gov/books/NBK379582/). Breachdyke (talk) 14:23, 26 June 2018 (UTC)
- Depending on trial entry criteria, design and execution it is possible to find statistically deemed benefit for practically anything. In the first of the references cited in the article lead in support of CBT/GET (yes GET is in this reference)/exercise therapy, it is conceded that: "This systematic review was limited by deficiencies of the trials. Most trials enrolled participants on the basis of case definitions for CFS only. The Oxford CFS case definition is the least restrictive, and its use as entry criteria could have resulted in selection of participants with other fatiguing illnesses or illnesses that resolve spontaneously with time (16, 71). The Institute of Medicine recently released new diagnostic criteria for CFS that require the presence of postexertional malaise, unrefreshing sleep, and either cognitive impairment or orthostatic intolerance (7, 72). Participants in previous trials did not meet these requirements." http://annals.org/aim/fullarticle/2322801/treatment-myalgic-encephalomyelitis-chronic-fatigue-syndrome-systematic-review-national-institutes. Breachdyke (talk) 10:22, 26 June 2018 (UTC)
- Compare the Cochrane review cited in the article lead: "Three studies used the Centers for Disease Control and Prevention (CDC) 1994 criteria (Fukuda 1994) as inclusion criteria (Jason 2007; Moss-Morris 2005; Wallman 2004), and five (Fulcher 1997; Powell 2001; Wearden 1998; Wearden 2010; White 2011) used the Oxford criteria ... All but one study (Wallman 2004) reported depression, which ranged from 18% (Wearden 2010) of those with a depression diagnosis to 39% among participants with a current Axis I disorder (Jason 2007)" (http://cochranelibrary-wiley.com/doi/10.1002/14651858.CD003200.pub7/full). Moreover, all of these trails were unblinded (something which the review describes as introducing a "high risk" of bias), and the only objective outcome measure reported on in the review was health resource usage in follow up data for one trial. Breachdyke (talk) 12:20, 26 June 2018 (UTC)
- It seems these walls of text are all saying the same thing: you want to overplay one source and downplay other sources according to a governing POV (roughly, that GET/CBD are bad). That's not going to happen because WP:NPOV is a core policy. I am tempted to say just drop the WP:STICK, but as a final effort could you at least do everyone the courtesy of succinctly proposing the exact change you want to make (i.e. "change X to Y" or "delete X"). This is what the page is meant to be for, and not general discussion / argumentation. Alexbrn (talk) 14:36, 26 June 2018 (UTC)
- It's because NPOV is a core policy that the article lead sentence re CBT and GET needs either balancing, or removing and left to the main article for discussion. By the way, "a gradual increase in activity suited to individual capacity " is how the Cochrane view you promote defines GET, so I'm calling it GET ("a negotiated, incremental increase in the duration of time spent physically active followed by an increase in intensity" (http://cochranelibrary-wiley.com/doi/10.1002/14651858.CD003200.pub7/full)). (And I believe CBT and GET can be extremely useful treatments; it depends on the disease). Breachdyke (talk) 18:18, 26 June 2018 (UTC)
- re the introduction: Even though advocates for CBT and exercise therapy are now more circumspect, they are therapies statistically deemed beneficial in studies for the patient cohort treated and supported by high impact secondary WP:MEDRS sources NHS[31], AHRQ[32], and Cochran[33] as previously discussed here at talk. I know of no other therapies that can be sourced like that. Ward20 (talk) 04:49, 24 June 2018 (UTC)
Fellow editors, I think I've identified the problem here. The article lead contains a positive sentence re CBT and GET but the supporting references are too problematic. For example, the Cochrane review concludes positively for CBT and GET yet says all the trials reviewed had a "high risk" of bias and five out the eight trial used diagnostic criteria which "could have resulted in selection of participants with other fatiguing illnesses or illnesses that resolve spontaneously with time". Indeed a significant proportion of trial participants had depression. The review clearly lacks internal consistency. There are also other reliable sources which contradict the sources quoted. So I fully agree with Rainywednesdays suggestion: "when the evidence for the efficacy of any particular treatment is so weak and contested, is there good reason to mention any of them in the introduction, where there will not be room to go into the details of the dispute and the reasons for ongoing uncertainty?" Let's leave out any claims re treatments from the article intro. Breachdyke (talk) 10:21, 27 June 2018 (UTC)
- The actual Cochrane conclusion does not say "weak and contested" but says "patients with CFS may generally benefit and feel less fatigued following exercise therapy, and no evidence suggests that exercise therapy may worsen outcomes". The lede summarizes the body, and draws on three sources (not just Cochrane) in any case. I think the current wording is properly reflective of the good sources cited: not too strong and not too skeptical. I disagree with the proposal to remove it. Alexbrn (talk) 10:31, 27 June 2018 (UTC)
- Agree with Alexbrn. The article only cites 3 sources for the lead wording on execise, but CDC agrees with the wording too.[34] Ward20 (talk) 14:26, 27 June 2018 (UTC)
- The disputed sentence in the article lead doesn't conform to WP:ASSERT (https://en.wikipedia.org/wiki/Wikipedia:Neutral_point_of_view/FAQ#Assert_facts,_not_opinions). As this talk page discussion shows, whether or not there is evidence suggesting that CBT and GET are effective in some ME/CFS cases is a matter of opinion not fact. There is not a scientific consensus on the factual status of the disputed sentence. To overcome this the sentence needs balancing (to show the range of significant opinion) or removing (or moving to the article main sections). Breachdyke (talk) 10:54, 29 June 2018 (UTC)
- There doesn't need to be "scientific consensus" except for claims of WP:RS/AC. What there is a consensus for (here) is that the lede properly summarizes accepted knowledge on this topic, in its current state. In lieu of new sources I think this matter is closed. Alexbrn (talk) 11:12, 29 June 2018 (UTC)
- Alexbrn, "the lede properly summarizes accepted knowledge on this topic". Accepted by whom? Not by AHRQ in their evidence review, who along with the NIH reject the Oxford criteria, (https://www.ncbi.nlm.nih.gov/books/NBK379582/). The CDC website recommends activity management, aka pacing, and makes no mention of GET (or any concept of planned incrementally increasing activity) or CBT (https://www.cdc.gov/me-cfs/treatment/index.html). It is also difficult to reconcile the article lead disputed sentence with the Dutch Health Council, who say refusing CBT and GET is not inadequate recovery behaviour (https://www.gezondheidsraad.nl/en/task-and-procedure/areas-of-activity/optimale-gezondheidszorg/mecfs). NICE are revising their guideline (https://www.nice.org.uk/news/article/nice-announces-next-steps-in-updating-its-guideline-on-me-cfs). Are you convinced this is a proper summary which represents "fairly, proportionately, and, as far as possible, without editorial bias, all of the significant views that have been published by reliable sources on a topic" (https://en.wikipedia.org/wiki/Wikipedia:Neutral_point_of_view)? Breachdyke (talk) 14:36, 29 June 2018 (UTC)
- There doesn't need to be "scientific consensus" except for claims of WP:RS/AC. What there is a consensus for (here) is that the lede properly summarizes accepted knowledge on this topic, in its current state. In lieu of new sources I think this matter is closed. Alexbrn (talk) 11:12, 29 June 2018 (UTC)
- The disputed sentence in the article lead doesn't conform to WP:ASSERT (https://en.wikipedia.org/wiki/Wikipedia:Neutral_point_of_view/FAQ#Assert_facts,_not_opinions). As this talk page discussion shows, whether or not there is evidence suggesting that CBT and GET are effective in some ME/CFS cases is a matter of opinion not fact. There is not a scientific consensus on the factual status of the disputed sentence. To overcome this the sentence needs balancing (to show the range of significant opinion) or removing (or moving to the article main sections). Breachdyke (talk) 10:54, 29 June 2018 (UTC)
- Agree with Alexbrn. The article only cites 3 sources for the lead wording on execise, but CDC agrees with the wording too.[34] Ward20 (talk) 14:26, 27 June 2018 (UTC)
The AHRQ Addendum (which is one in the same concerning NIH referred to above as far as I can see)[35] finds a "low strength of evidence that CBT improves outcomes of fatigue" when excluding CBT Oxford studys, and insufficient or negative results for other measures of the illness. Excluding Oxford in future studies is recommended, but they don't say the studies are wrong, just biased to the population they studied, and a place to start from. The CDC does support the wording for exercise that is in the lead, "Patients who have learned to listen to their bodies might benefit from carefully increasing exercise to improve fitness and avoid deconditioning." The lead doesn't even mention GET except to say patients are negative about it. The Dutch Health Council basically said patients that reject CBT and GET are not considered to be trying to avoid recovery when applying for benefits. That says nothing about persons that may benefit from CBT or GET. NHS is revising their guidelines, so what, no one knows what they will say. The article does present the opposing positions in the body of the article. That is what WP:NPOV requires. Honestly, I think the lead wording is well supported by the sources given. All I have seen to rebut is repeditive, very weak, and would give a WP:FALSEBALANCE. When or if sources change, the article will change, simple. Ward20 (talk) 17:20, 29 June 2018 (UTC)
- Ward20, Concerning the AHRQ and NIH, when you say "they don't say the studies are wrong, just biased to the population they studied", the Wikipedia article lead must note that bias, otherwise it is itself biased. Breachdyke (talk) 17:39, 5 July 2018 (UTC)
- Note that when the article lead says "...can be beneficial in some cases" it's clearly meaning a subset of cases of ME/CFS, but AHRQ and NIH say the Oxford criteria entail "a high risk of including patients who may have an alternate fatiguing illness or whose illness resolves spontaneously with time" (https://www.ncbi.nlm.nih.gov/books/NBK379582/). In other words, AHRQ and NIH refute the sentence in the article lead insofar as it relies on sources which rely in turn, to any significant degree, on Oxford based studies. The sources concerned do rely on the Oxford criteria to a significant degree. Breachdyke (talk) 17:57, 5 July 2018 (UTC)
- The material you are rehashing is already in the Exercise therapy section where it belongs, not the lead. Ward20 (talk) 23:24, 5 July 2018 (UTC)
- The problem here is that CFS has many definitions, some of which barely overlap. A statement regarding the efficacy of any treatment is meaningless when this isn't taken into account. Yet the article attempts to treat all these different target groups as one, without even mentioning so. Saint Jut (talk) 22:08, 8 July 2018 (UTC)
- The material you are rehashing is already in the Exercise therapy section where it belongs, not the lead. Ward20 (talk) 23:24, 5 July 2018 (UTC)
Age of onset
The article currently says that ME/CFS "typically starts between 40 and 60 years of age", citing a CDC webpage which states that "while most common in people between 40 and 60 years old, the illness affects children, adolescents, and adults of all ages."
However, if you look at Figure 1 from this 2014 study of 5,809 patients, they observed two age peaks in the onset of this illness, a first peak in the age group of 10 to 19 years and a second peak in the age group of 30 to 39 years. Hip-IV (talk) 01:36, 8 September 2018 (UTC)
- The CDC is a secondary source. The 2014 Norway study appears to be a primary source. Unless an important reliable secondary source publishes an evaluation of the Norway 2014 figure 14 data, the CDC source has precedence according to WP:MEDRS. Ward20 (talk) 04:31, 8 September 2018 (UTC)
- The CDC may be secondary, but it is not reliable. It has an agenda. The Norway study isn't much of a help either though. The reason is that they conflate ME and CFS (in Norway, CFS is incorrectly registered as G93.3). The first is responsible for the later peak, the second for the earlier peak. Note furthermore that peak age of prevalence is not the same as peak age of incidence. Sporadic ME most often starts between 30 and 40. Saint Jut (talk) 16:29, 9 September 2018 (UTC)
- "not reliable"? "Agenda"? Alexbrn (talk) 12:22, 12 September 2018 (UTC)
- The CDC may be secondary, but it is not reliable. It has an agenda. The Norway study isn't much of a help either though. The reason is that they conflate ME and CFS (in Norway, CFS is incorrectly registered as G93.3). The first is responsible for the later peak, the second for the earlier peak. Note furthermore that peak age of prevalence is not the same as peak age of incidence. Sporadic ME most often starts between 30 and 40. Saint Jut (talk) 16:29, 9 September 2018 (UTC)
Chronic fatigue syndrome synonyms
Please use this space to provide major sources that say CFS is not a synonym to the other names concering this change [36] Ward20 (talk) 07:14, 12 September 2018 (UTC)
- The burden of proof belongs to the other side. Point is, the IOM report, to which this was sourced, doesn't say this, and there should not be an unsourced claim of this magnitude in the infobox. Saint Jut (talk) 07:29, 12 September 2018 (UTC)
Regardless, we have, to begin with:
- the ICD10 where PVFS is an umbrella term, the group header of G93.3 to which ME belongs, i.e. the relation between these terms is hierarchical;
- Ramsay discussing whether ME is a PVFS or not (again indicating that PVFS is a more general term);
- the ICD10-CM with different codes for ME (at G93.3) and CFS (R53.82);
- the current proposal for the ICD11 with different codes for ME and neurological CFS;
- the IOM stressing that ME and CFS are different conditions, and then concluding that neither myalgia nor encephal(omyel)itis is characteristic for the combined group which it was ordered to investigate.
The term CFIDS was coined by patients exactly because they felt CFS wasn't accurately describing their condition. There is no medical source either way that I'm aware of, but it is a gotspe to list it as synonymous anyway. Saint Jut (talk) 08:38, 12 September 2018 (UTC)
- The IOM source[37] talks about ME, CFS, PVFS, as the literature search and common terms used to describe the illness for their research on pgs. 20,29,30. SEID is described in the Society and culture/Naming section of this article. CFIDS goes back aways to when there was a daughter article for alternative names[38].
- Where exactly does the IOM state, "the IOM stressing that ME and CFS are different conditions, and then concluding that neither myalgia nor encephal(omyel)itis is characteristic for the combined group which it was ordered to investigate"? Not saying it doesn't, but I don't feel like reading 200 pages to find it. Thanks. Ward20 (talk) 09:33, 12 September 2018 (UTC)
- It's not a quote. It is probably a good idea to read the report in its entirety, because it's sort of a game changer but frequently gets misquoted. Using a variety of search terms is already an indication that these terms are not synonymous, otherwise one search term would suffice (the search engine takes synonyms into account). But it gets more explicit than that. The question to answer is, however, the opposite. Where does it say the terms are synonymous? Saint Jut (talk) 11:47, 12 September 2018 (UTC)
- Page 1 of the summary: "For the purposes of this report, the umbrella term “ME/CFS” is used to refer to both conditions." (my bold) Saint Jut (talk) 12:12, 12 September 2018 (UTC)
"the current proposal for the ICD11 with different codes for ME and neurological CFS"
As far as I can see[39] ICD-11 retains the PVFS-ME-CFS conflation found in the vanilla ICD-10. Little pob (talk) 11:17, 12 September 2018 (UTC)- This is not the most detailed information, but nonetheless it shows that the terms are not synonymous. In this table, PVFS is the name of a group of conditions. ME and (neurological) CFS are two different conditions under that umbrella (not shown is that they're expected to each get a subcode). This is the first time that CFS gets a code in the WHO's classification. Saint Jut (talk) 11:47, 12 September 2018 (UTC)
- @Saint Jut:
"they're expected to each get a subcode"
the current published beta for ICD-11 has no "subcodes" for the listed inclusion terms at 8E49. If it did it would have an expandable branch on the left pane (cf. 8E4A). So if you know of a proposal to add subcodes, please provide a source. With regards to CFS in ICD-10; whilst it might not be mentioned as an includes at G93.3, the index (volume 3) does send you there. Little pob (talk) 12:33, 12 September 2018 (UTC)- It does, but if you read the reading instructions included in the ICD, you will understand that this doesn't mean anything beyond 'maybe look there'. Synonyms are always included in the table itself. The detailed info on the ICD11 isn't commonly available but that has no baring on this discussion. Maybe now would be a good time to tell us what you think about the article text? Saint Jut (talk) 12:49, 12 September 2018 (UTC)
It does, but if you read the reading instructions included in the ICD, you will understand that this doesn't mean anything beyond 'maybe look there'.
If it were a "see also" type trail I would agree; however, it's not. You are explicitly sent to G93.3 by the index, and – once you get to the tabular to verify – there are no excludes to say that you are at the wrong code. (Presumably ICD-10-CM will though, as it has R53.82 for CFS.) So there is no other code available in the base version of ICD-10 for these terms. But I won't hide from the fact that, as a classification, the ICD does "lump" conditions together (e.g. all types of pulmonary fibrosis are coded to J84.1.) <aside>Out of interest, are you involved in coding/billing/nosology? (BTW that isn't an "I'm an expert" rhetorical question. I'm asking because there could well be the potential for any differing national standards to get in the way of us coming to an agreement on this specific point on indexing, cross-references, includes, excludes etc.)</aside>The detailed info on the ICD11 isn't commonly available but that has no baring on this discussion.
I would counter that it does have baring. Specifically to your fourth point above that ICD-11 proposes "different codes for ME and neurological CFS". This is because the current, publicly available draft does not support that claim.Maybe now would be a good time to tell us what you think about the article text?
Not sure what that would prove, but OK... I don't have an opinion on the article. I've not read enough of it to form one! (Probably not what you expected.) What I will say is; I have previously had stress-induced fatigue, and can empathise with CFS/ME/PVFS patients. If you're wondering why it is that I'm chiming in, it's because this specific thread relates to ICD. Little pob (talk) 18:15, 12 September 2018 (UTC)
- It does, but if you read the reading instructions included in the ICD, you will understand that this doesn't mean anything beyond 'maybe look there'. Synonyms are always included in the table itself. The detailed info on the ICD11 isn't commonly available but that has no baring on this discussion. Maybe now would be a good time to tell us what you think about the article text? Saint Jut (talk) 12:49, 12 September 2018 (UTC)
- @Saint Jut: {“ME/CFS” is used to refer to 'both conditions'} This is because they are working with two separate definitions that describe conditions with similar symptoms that may or may not identify the same disease (IOM page 1). Nevertheless, later they recommend a new definition and name, SEID to replace 'both conditions', indicating they lump them all together as of 2015 (IOM page 5).Ward20 (talk) 16:17, 12 September 2018 (UTC)
- Only to replace CFS. The IOM doesn't suggest to replace ME. More importantly, their advice wasn't followed. Both ME and CFS are still alive, and SEID is not. Preliminary research by Jason shows that it's hopeless as an alternative. Saint Jut (talk) 16:47, 12 September 2018 (UTC)
- I disagree the IOM report doesn't suggest to only replace CFS, they consistently refer to replacing "ME/CFS" with a new defintion and name. I do agree their recommendation hasn't been popular or implemented.Ward20 (talk) 17:18, 12 September 2018 (UTC)
- Only to replace CFS. The IOM doesn't suggest to replace ME. More importantly, their advice wasn't followed. Both ME and CFS are still alive, and SEID is not. Preliminary research by Jason shows that it's hopeless as an alternative. Saint Jut (talk) 16:47, 12 September 2018 (UTC)
- @Saint Jut:
- This is not the most detailed information, but nonetheless it shows that the terms are not synonymous. In this table, PVFS is the name of a group of conditions. ME and (neurological) CFS are two different conditions under that umbrella (not shown is that they're expected to each get a subcode). This is the first time that CFS gets a code in the WHO's classification. Saint Jut (talk) 11:47, 12 September 2018 (UTC)
ICD 11 is fairly clear that these are often used interchangeably. https://icd.who.int/browse11/l-m/en#/http%3a%2f%2fid.who.int%2ficd%2fentity%2f569175314 Doc James (talk · contribs · email) 19:35, 12 September 2018 (UTC)
- "SEID should replace myalgic encephalomyelitis/chronic fatigue syndrome for patients who meet the criteria set forth in this report" (page 11)
I.e., it should replace the umbrella term. Note furthermore that ME patients generally do not meet SEID criteria, since these were derived from the larger group where ME is a small minority.
- "In what will likely be its most controversial recommendation, the committee has proposed that the name “chronic fatigue syndrome” no longer be used to describe this disorder. The committee repeatedly heard from patients that this term was stigmatizing and too often precluded their receiving appropriate care. The committee instead determined that the name “systemic exertion intolerance disease” (SEID) better characterizes the disorder for which its proposed diagnostic criteria were developed." (page 228)
So 'ME/CFS' is out, and 'CFS' must go. ME, however, remains. Saint Jut (talk) 19:58, 12 September 2018 (UTC)
- From a book from a few years ago.https://www.ncbi.nlm.nih.gov/books/NBK284910/
- It appears WHO has disagreed. Doc James (talk · contribs · email) 20:02, 12 September 2018 (UTC)
- Not in your source, just like in your previous comment your source doesn't contain what you claim it does. I figure that we now know how some of the misreferences in the article entered the text. Saint Jut (talk) 20:14, 12 September 2018 (UTC)
New book criticizes the PACE trial
You might be interested to learn that academic psychologist Professor Brian Hughes has just published a book "Psychology in Crisis" (ie, a tertiary source) about the way flawed research prospers so freely in modern psychology. This book contains a whole chapter on the PACE trial of CBT and GET as an example of alarmingly bad research, and thus may be relevant for this CFS article, which currently has large sections on CBT and GET.
This new book joins a growing body of academic criticism of the methodology and conclusions of the PACE trial, including:
• Rebecca Goldin, director of Stats.org and Professor of Mathematical Sciences: she concludes: "the flaws in this design were enough to doom its results from the start".
• Professor James Coyne, psychologist: "The data presented are uninterpretable".
• Professor Vincent Racaniello, virologist: "PACE study is a sham, with meaningless results. In this case, the emperor truly has no clothes".
• Sonia Lee, clinical epidemiologist: she concludes: "rectify, or retract findings".
• Sten Helmfrid and Johan Edsberg: "Time to Reject the PACE Study".
• Dr Ellen Goudsmit, retired health psychologist: "A treatment like GET is simply not appropriate for a disease like ME which is linked to infection and metabolic abnormalities. Given the close relationship between exertion and symptoms, it follows that asking a patient to increase their activity levels is as logical as advising smokers with lung cancer to gradually increase the number of cigarettes they smoke".
• David Tuller, lecturer at University of California, Berkeley: "The study included a bizarre paradox: participants’ baseline scores for the two primary outcomes of physical function and fatigue could qualify them simultaneously as disabled enough to get into the trial but already 'recovered' on those indicators–even before any treatment. In fact, 13 percent of the study sample was already 'recovered' on one of these two measures at the start of the study".
• Professor Andrew Gelman, Professor of statistics and political science at Columbia University: "One thing that struck me about this PACE scandal: if this study was so bad as all that, how did it taken so seriously by policymakers and the press? There’s been a lot of discussion about serious flaws in the published papers, and even more discussion about the unforgivable refusal of the research team to share their data. But the question I want to address here is, how did they get into the position where this research got taken seriously in the first place?"
For other academic critics of PACE, see the MEpedia page on PACE.
91.125.89.41 (talk) 00:57, 31 August 2018 (UTC)
- We are looking for medical textbooks as sources. Doc James (talk · contribs · email) 17:16, 17 September 2018 (UTC)
Views of patient groups
This sentence: "Patient groups have criticized the use of CBT and graded exercise therapy (GET)" was changed to:
"A minority of patient groups reject any psychological component[1] and some have criticized the use of CBT and graded exercise therapy (GET).[2]"
Even ignoring the problem of using the Science Media Centre as a source for anything other than the views of the Science Media Centre, the page linked to does not even claim that "A minority of patient groups reject any psychological component". It certainly does not detail exactly which patient groups supposedly "reject any psychological component". There is a long history of unpleasant prejudices about ME/CFS patients, and attempts to present patient concerns about the way CBT and GET are promoted as being a result of 'anti-psychiatry' or a rejection of 'any psychological component'. These prejudices only seem to be promoted by those who fail to understand the problems with research like the PACE trial. Back in 1999 a paper from Simon Wessely stated that: "The stereotype of CFS sufferers as perfectionists with negative attitudes toward psychiatry was not supported."
Criticism of the claims made for CBT and GET is not just from a small minority rejecting "any psychological component": all major UK patient charities are now signatories of the open letter raising concerns about the PACE trial and calling for an independent investigation: http://www.virology.ws/2018/08/13/trial-by-error-open-letter-to-the-lancet-version-3-0/
I am going to change this sentence back to how it was.Rainywednesday (talk) 03:50, 18 September 2018 (UTC)
References
- ^ "CFS/ME – The illness and the controversy | Science Media Centre". www.sciencemediacentre.org. Science Media Centre. Retrieved 26 August 2018.
- ^ Elgot, Jessica (18 October 2015), "Chronic fatigue patients criticise study that says exercise can help", The Guardian, retrieved 20 June 2018
- The source says "Some people do not accept that psychological factors play a role in the illness or its treatment and dispute many aspects of the evidence that supports CBT and GET as treatments. Some also claim that these treatment are harmful. A minority have engaged in activities designed to actively disrupt such research." so WP:V seems stisfied. This is a fairly commonplace observation, no? Alexbrn (talk) 06:59, 18 September 2018 (UTC)
- Lots of prejudices are commonplace. That is part of the problem with them. Nasty old 'stereotypes' (as Wessely put it) about CFS patients can encourage people unable (or unwilling) to understand the problems with research like PACE to imagine that they have some understanding of the controversies surrounding the condition, but we all have a responsibility to look carefully at the evidence and not allow ourselves to be caught up in bigotry.
- The Science Media Centre described the PACE trial as "the first definitive comparison of various treatments for CFS/ME". It is difficult to consider them an unbiased source on this topic.
- "Some people" is not "A minority of patient groups".
- Which people? Are they noteworthy? Where have they made these claims? Why should a claim related to this be inserted into a sentence about patient groups criticising the use of CBT and GET?
- If you wish to refer to the Science Media Centre's claims about CFS, then the only secondary source I can find on that relates to concerns that the Science Media Centre has played a role in the promotion of misleading information in the UK: https://www.independent.co.uk/news/long_reads/why-patients-me-demanding-justice-millions-missing-chronic-fatigue-illness-disease-a8133616.html Rainywednesday (talk) 12:58, 18 September 2018 (UTC)
- What are you on about? What matters here is reflecting accepted knowledge about CFS. That some people are opposed on principle to acknowledging the possibly psychological aspects is just such knowledge, and it central to much of the "controversy". If you continue to edit war, you risk getting blocked. Alexbrn (talk) 13:57, 18 September 2018 (UTC)
- If you wish to refer to the Science Media Centre's claims about CFS, then the only secondary source I can find on that relates to concerns that the Science Media Centre has played a role in the promotion of misleading information in the UK: https://www.independent.co.uk/news/long_reads/why-patients-me-demanding-justice-millions-missing-chronic-fatigue-illness-disease-a8133616.html Rainywednesday (talk) 12:58, 18 September 2018 (UTC)
- "Some Jews attempt to corruptly manipulate the media in order to mislead the general public" - do you understand why it would be problematic to insert this claim into the lede of a wikipedia article? I think that there is good reason to be cautious about making stigmatising claims about 'some people with CFS' or 'some Jews', and that specific examples of who you mean should be provided rather than the use of vague assertions. That you appear to not understand this raises serious questions about whether you are a fit person to be editing articles on this topic.
- I explained why the Science Media Centre should not be viewed as an unbiased source on this topic, and you failed to explain why you disagreed. Also, the page you linked to does not claim that "Some people with CFS reject any psychological component".
- I reverted an unjustified change to the article and explained why. I do not see why my change should be considered any more of an 'edit war' than yours.Rainywednesday (talk) 14:22, 18 September 2018 (UTC)
- Your Jew comment is specious racism; OTOH, it is well documented and true that the vocal, even aggressive, patient-advocate lobby for CFS holds certain views and Wikipedia faithfully follows RS in reporting this knowledge. Alexbrn (talk) 21:18, 18 September 2018 (UTC)
- Your comment suggests you are unaware of the fact that lots of people attempt to corruptly manipulate the media in order to mislead the general public, and that while many are not, some of these people are Jewish. One need only observe how anti-Semites jump upon examples like Harvey Weinstein to see how bigots try to amplify the importance of the worst behavior of 'some Jews'. Of course, this does not justify a vague and stigmatising sentence that plays into old bigotries being inserted into the lede of a wikipedia article.
- You've failed to offer any substantive reason why the comment which played into anti-Semitic bigotry should be seen as any less acceptable than the comment you wanted inserted into the lede of this article, which played into bigoted views of ME/CFS patients. You also failed to explain why you thought that relying on a webpage that failed to make the claims made in your sentence, and was from a source with a history of promoting misleading information on this topic, was sufficient for promoting this stigmatising narrative.
- Sadly, many anti-Semites do not realise that they are ignorant bigots, instead believing that they are just reporting well documented facts about an unpleasant and aggressive minority group which hold dangerous views that need to be faithfully reported. While there is a growing awareness of the danger of promoting stigmatizing and prejudiced narratives about minority groups, some people still fail to appreciate their moral responsibilities here.
- The reason you gave for inserting your last reply was "almost too stupid a comment to respond to, but...". It seems that you failed to understand my comment, and that your reply was not well considered. I would suggest that in the future you avoid making public your attempts to judge whether or not other people's comments are stupid.Rainywednesday (talk) 16:59, 5 October 2018 (UTC)
- What an unpleasant editor that is. Do we have to put up with people like that, or are they disruptive enough already? -Roxy, in the middle. wooF 17:15, 5 October 2018 (UTC)
- Can you point to anything I've said that is unreasonable or inaccurate? Sadly, some people just find the truth unpleasant.Rainywednesday (talk) —Preceding undated comment added 13:22, 17 October 2018 (UTC)
Whether or not a minority of sufferers reject any psychological factors it is not relevant to this page. Secondary the sources are not strong enough to warrant inclusion. It should be reverted. C7762 (talk) 14:57, 18 September 2018 (UTC)
- It's a significant amount of sufferers (see the various research into this), and it seems to be one of the most important issues regarding the illness. --sciencewatcher (talk) 19:36, 18 September 2018 (UTC)
- The problem I have with the way it is presently stated in the lead is that there is no way for the reader to know exactly where or why some patients object to the psychological factors.
- The short answer about the psychological aspects: there are largely different approaches and definitions between the research in the UK and the research in the US. This has led to difficulties in the ability of patients to receive medical, social, and financial support when they become ill. It's very much dependent on whether the disease is viewed as psychological or physical. It's not right that a mental disorder is treated differently, but it's a fact it is.
- The long answer is much more complicated, with all sorts of competing interests using the illness for their own benefit for the past 30 plus years. A WP:NPOV description of this material would have to be be much more complicated, detailed, and comprehensive than what is in the lead.
- The lead is not supposed to summarize something not explained in the body of the article, and as far as I can see a NPOV of some patients rejection of psychological factors is not included in the article. Ward20 (talk) 23:47, 18 September 2018 (UTC)
- You're right. I've moved that sentence from the lead to the controversy section. I think it's true that most patient groups now oppose CBT and GET, but the current ref doesn't support that so I'm leaving it for now. --sciencewatcher (talk) 06:54, 19 September 2018 (UTC)
- It's probably something that should be expanded upon, but it would be a lot of careful work to keep it NPOV because of the polarization of the subject. Ward20 (talk) 07:37, 19 September 2018 (UTC)
- This has turned out to be a timely discussion in regards to two new sources: Graded exercise therapy for myalgic encephalomyelitis/chronic fatigue syndrome is not effective and unsafe. Re-analysis of a Cochrane review (October 8 2018)[40], and Exclusive: Science journal to withdraw chronic fatigue review amid patient activist complaints (October 18 2018)[41] Hopefuly, using reliable sources, reasons for rejection of psychological factors may be further explained in a NPOV way. Ward20 (talk) 10:45, 19 October 2018 (UTC)
- I don't think Health Psychol Open is a reliable journal, or this paper by Mark Vink a reliable paper, for our purposes. Agreed Cochrane's "temporary withdrawal" (whatever that means) need to be covered neutrally. Alexbrn (talk) 10:55, 19 October 2018 (UTC)
- This has turned out to be a timely discussion in regards to two new sources: Graded exercise therapy for myalgic encephalomyelitis/chronic fatigue syndrome is not effective and unsafe. Re-analysis of a Cochrane review (October 8 2018)[40], and Exclusive: Science journal to withdraw chronic fatigue review amid patient activist complaints (October 18 2018)[41] Hopefuly, using reliable sources, reasons for rejection of psychological factors may be further explained in a NPOV way. Ward20 (talk) 10:45, 19 October 2018 (UTC)
PVFS
Ah, somebody has kindly tidied up my comment here but my point was that a wikipedia search for PVFS leads to this article but the introduction seems contradictory to the very existence of PVFS. M.E. also also leads here, in the UK an old definition of M.E. was PVFS that had lasted more than 6 months. I'm not planning to edit the article as I'm open to accusations of 'POV' & 'original research' etc but I'm suggesting that either PVFS should lead to a page of it's own - where it's existence/non-existence or obsoleteness could be explained or else the intro to the current article needs re-writing. V86.150.252.216 (talk) 12:26, 23 October 2018 (UTC)
As well as enterovirus triggered illnesses, the long term effects some people experience following exposure to organophosphates are also labelled CFS in the UK. Isn't the truth that if 'CFS' has any meaning at all then it may appear to be linked to a previous condition or CFS may appear where no prior condition has been noted but really we just don't know? the wording "Is not due to" just seems a little prejudicial as an opener on a subject where much is unproven. V86.166.105.49 (talk) 11:27, 7 October 2018 (UTC).
- You are correct that neither PVFS nor ME should lead here. CFS belongs in R53 which is fatigue / malaise of unknown cause, excluding PVFS (and hence also ME). Saint Jut (talk) 20:57, 17 December 2018 (UTC)
BBC news story
https://www.bbc.co.uk/news/health-46570494 You're welcome. 25 years ago anybody who actually knew anything at all about M.E. knew there were types where the immune system was underactive & types where the immune system was overactive, but some people didn't want to listen. Now it's like it's all newly discovered! V86.160.155.46 (talk) 11:55, 17 December 2018 (UTC)
- Not reliable for our purposes. Alexbrn (talk) 12:29, 17 December 2018 (UTC)
- Interesting but it's a small study, and unconfirmed. Including such a result would be premature. It does connect though to the general notion that CFS should not be given to patients as a clinical diagnosis. Patients satisfying CFS criteria should be examined further. Missing Hepatitis C or any 'underlying' disease is not what we want. It would be nice if we had a reliable source for this view. Saint Jut (talk) 21:07, 17 December 2018 (UTC)
- Confirms my long-standing view: some people are sick. There are a lot of different causes. Encephalomyelitis is unlikely to be the cause in a lot of these cases. Chronic fatigue syndrome is a more correct name until we know the actual cause. Guy (Help!) 00:46, 18 December 2018 (UTC)
- My reading of the news article is that interferon makes people feel iffy, and that this iffiness continues after cessation of the administration. I am puzzled why this touted as evidence one way or the other for anything because pharmacological grade interferon cannot be compared to the cytokine milieu during a normal infective illness. JFW | T@lk 07:27, 18 December 2018 (UTC)
Archiving after 21 days due to "controversial nature of topic"
- 21 days seems a rather short time period to archive the talk pages. I was going to boldly change it, however there was a tag in the "edit source" that says the following: Please DO NOT CHANGE archiving settings without discussion on the talk page - these are chosen specifically due to the controversial nature of the subject matter.
- I could be wrong, but being controversial is not a justification for archiving so frequently. As per WP:TALKCOND the time period should be chosen based on length of the talk page. 3 months is common for a low volume page such as this.Dig deeper talk 01:26, 21 December 2018 (UTC)
- Looked through the talk page archives. Seems the talk page is not as active as it once was. Nevertheless, I changed my mind. 21 days is fine here. Dig deeper talk 01:38, 21 December 2018 (UTC)
Evidence suggests
The following discussion is closed. Please do not modify it. Subsequent comments should be made on the appropriate discussion page. No further edits should be made to this discussion.
Alexbrn Statement reads - "Evidence suggests that cognitive behavioral therapy (CBT) and a gradual increase in activity suited to individual capacity can be beneficial in some cases"... Except that the evidence is predominately based on a discredited study and while it may have some benefit, it may not because the evidence is, at best, negligible statistically speaking. Later the article goes on to say:
"A report by the Institute of Medicine published in 2015 states that it is unclear whether CBT helps to improve cognitive impairments experienced by patients." "The authors concluded that, as this finding is contrary to the cognitive behavioural model of CFS, patients receiving CBT were adapting to the illness rather than recovering from it." "that CBT in its current form should not be recommended as a primary intervention for people with CFS" "As with CBT, patient organisations have long criticised the use of exercise therapy, most notably GET, as a treatment for CFS.[98] In 2012 the MEA commenced an opinion survey of patients who had received GET. Based on the findings of this survey, in 2015 the MEA concluded that GET in its current delivered form should not be recommended as a primary intervention for persons with CFS."
Thus this sentence needs to change because it suggests that CBT and GET are possible treatments for some cases where as the evidence and current treatments say they are not.Leaving this overview in place gives an erroneous statement about the current medical understanding. It has to change. By reverting, the Wikipedia entry is in error. ☕ Antiqueight chatter 17:48, 18 February 2019 (UTC)
- You have cherry-picked the body text you quote to omit the positive side of CBT. Overall this is consistent with the lede which accurately relays the fact that there is suggestive evidence that CBT is "beneficial in some cases". Alexbrn (talk) 17:57, 18 February 2019 (UTC)
- Current evidence suggests there is no beneficial side to CBT other than possibly making a very small percentage feel better about the fact that they feel awful and that the number who feel better is about the same as those who get no CBT. If the article further suggests CBT has a real supported benefit then it is also incorrect. ☕ Antiqueight chatter 18:17, 18 February 2019 (UTC)
- Also - I didn't cherry pick - those are just about the only places where CBT is mentioned in the article. ☕ Antiqueight chatter 18:18, 18 February 2019 (UTC)
- If there is current evidence to refute what the article says, you should have no problem providing refs. -Roxy, the dog. wooF 18:20, 18 February 2019 (UTC)
- Apart from anything else the evidence is cited in the current article. I was merely adjusting the overview to match the information in the body. But I did give a citation which granted wasn't to the papers in question but which does cite the papers in question. I didn't want to overload the sentence with citations like
- "No 'Recovery' in PACE Trial, New Analysis Finds". www.virology.ws.
- "(PDF) The PACE Trial Invalidates the Use of Cognitive Behavioral and Graded Exercise Therapy in Myalgic Encephalomyelitis/ Chronic Fatigue Syndrome: A Review". ResearchGate.
- "TRIAL BY ERROR: The Troubling Case of the PACE Chronic Fatigue Syndrome Study". www.virology.ws.
- ☕ Antiqueight chatter 11:02, 19 February 2019 (UTC)
- Yes but you can't just negate the finding as recorded in a recent Cochrane systematic review - which is about the strongest possible medical source. Our job here is duly to reflect the best sources, not advance some particular POV. Alexbrn (talk) 11:34, 19 February 2019 (UTC)
- Indeed not - but even the Cochrane reviews are tentative about suggesting the level of benefit and nothing in the rest of the article supports a positive statement about CBT and GET. At best the sentence should read "Evidence suggests that cognitive behavioral therapy (CBT) and a gradual increase in activity suited to individual capacity might be beneficial in some cases".And even then, the evidence suggests it is a long shot. ☕ Antiqueight chatter 20:54, 19 February 2019 (UTC)
- Alxbrn said: "Yes but you can't just negate the finding as recorded in a recent Cochrane systematic review - which is about the strongest possible medical source. Our job here is duly to reflect the best sources, not advance some particular POV." What recent Cochrane review are you talking about? The 2014 Larun review of exercise therapy has recently had this note attached:
- 'The author team has re‐submitted a revised version of this review following the complaint by Robert Courtney. The Editor in Chief and colleagues recognise that the author team has sought to address the criticisms made by Mr Courtney but judge that further work is needed to ensure that the review meets the quality standards required, and as a result have not approved publication of the re‐submission. The review is also substantially out of date and in need of updating.
- Cochrane recognises the importance of this review and is committed to providing a high quality review that reflects the best current evidence to inform decisions.
- The Editor in Chief is currently holding discussions with colleagues and the author team to determine a series of steps that will lead to a full update of this review. These discussions will be concluded as soon as possible'.
- I hope that no-one would describe such a review, the problems with which have been so clearly explained and accepted by Cochrane's Editor in Chief, as "recent" and "about the the strongest possible medical source". That would be to push a truly misguided POV.
- For those who don't feel able to read the Cochrane review, Hilda Bastian recently blogged on some of the controversies surrounding it: https://blogs.plos.org/absolutely-maybe/2019/02/08/consumer-contested-evidence-why-the-me-cfs-exercise-dispute-matters-so-much/Rainywednesday (talk) 01:15, 21 February 2019 (UTC)
- I am aware (and it's been discussed here) that the review is controversial. However despite the kerfuffle (and false claims to the contrary) it was not withdrawn. We go by MEDRS, not blogs. If and when it gets updated, we will follow. It may of course not go in the direction many advocates are pressing for! Alexbrn (talk) 06:36, 21 February 2019 (UTC)
- And yet according to the rest of this article and the citations within it, including Cochrane and multiple sources not mentioned it is not really true to say that these "can be" when the evidence suggests "might possibly". ☕ Antiqueight chatter 08:32, 21 February 2019 (UTC)
- To repeat, we don't suppress good sources to promote some POV. I suggest we're done here. Alexbrn (talk) 08:47, 21 February 2019 (UTC)
- No one is suggesting suppressing - or even removing - the sources. Just making the overview agree with the rest of the article. ☕ Antiqueight chatter 11:43, 21 February 2019 (UTC)
- It does: there is a body of evidence suggesting the benefit of CBT/Exercise. We reflect that in the body and the lede. Alexbrn (talk) 12:15, 21 February 2019 (UTC)
- So what "recent" Cochrane review were you talking about Alexbrn?
- I was not suggesting citing Hilda Bastian's blog here, but thought that it could be a useful introductory piece for those who do not understand how Cochrane works, or who believe that the Larun review is merely "controversial", rather than having clearly breached Cochrane's own guidelines.Rainywednesday (talk) 12:58, 21 February 2019 (UTC)
- PMID 28444695. It's one of several sources on the topic that we cite within the 5 year window recommended by WP:MEDRS. Alexbrn (talk) 13:07, 21 February 2019 (UTC)
- "The 2016 one" - what 2016 one? It sounds as if you do not understand how Cochrane works, or how their reviews are dated?Rainywednesday (talk) 13:17, 21 February 2019 (UTC)
- From Alexbrns' 'reason for edit': "it is 2017, this one". That is the 2014 review. The only updates since then have been the addition of comments showing that the review includes inaccuracies and did not follow Cochrane's own guidelines, and then the addition of the editorial not quoted above, which describes it as "substantially out of date and in need of updating" and also says that even when the review authors had tried to correct their false claims with a resubmission, it was still not judged to be fit for publication as "further work is needed to ensure that the review meets the quality standards required, and as a result have not approved publication of the re‐submission". Each time comments are added to the review it is republished with the current date, but this does not make the review itself any more "recent". This can be confusing for the sort of people who cite a review without taking the time to read it first. Rainywednesday (talk) 13:26, 21 February 2019 (UTC)
- PMID 28444695. It's one of several sources on the topic that we cite within the 5 year window recommended by WP:MEDRS. Alexbrn (talk) 13:07, 21 February 2019 (UTC)
- It does: there is a body of evidence suggesting the benefit of CBT/Exercise. We reflect that in the body and the lede. Alexbrn (talk) 12:15, 21 February 2019 (UTC)
- No one is suggesting suppressing - or even removing - the sources. Just making the overview agree with the rest of the article. ☕ Antiqueight chatter 11:43, 21 February 2019 (UTC)
- To repeat, we don't suppress good sources to promote some POV. I suggest we're done here. Alexbrn (talk) 08:47, 21 February 2019 (UTC)
- And yet according to the rest of this article and the citations within it, including Cochrane and multiple sources not mentioned it is not really true to say that these "can be" when the evidence suggests "might possibly". ☕ Antiqueight chatter 08:32, 21 February 2019 (UTC)
- I am aware (and it's been discussed here) that the review is controversial. However despite the kerfuffle (and false claims to the contrary) it was not withdrawn. We go by MEDRS, not blogs. If and when it gets updated, we will follow. It may of course not go in the direction many advocates are pressing for! Alexbrn (talk) 06:36, 21 February 2019 (UTC)
- Alxbrn said: "Yes but you can't just negate the finding as recorded in a recent Cochrane systematic review - which is about the strongest possible medical source. Our job here is duly to reflect the best sources, not advance some particular POV." What recent Cochrane review are you talking about? The 2014 Larun review of exercise therapy has recently had this note attached:
- Indeed not - but even the Cochrane reviews are tentative about suggesting the level of benefit and nothing in the rest of the article supports a positive statement about CBT and GET. At best the sentence should read "Evidence suggests that cognitive behavioral therapy (CBT) and a gradual increase in activity suited to individual capacity might be beneficial in some cases".And even then, the evidence suggests it is a long shot. ☕ Antiqueight chatter 20:54, 19 February 2019 (UTC)
- Yes but you can't just negate the finding as recorded in a recent Cochrane systematic review - which is about the strongest possible medical source. Our job here is duly to reflect the best sources, not advance some particular POV. Alexbrn (talk) 11:34, 19 February 2019 (UTC)
- Apart from anything else the evidence is cited in the current article. I was merely adjusting the overview to match the information in the body. But I did give a citation which granted wasn't to the papers in question but which does cite the papers in question. I didn't want to overload the sentence with citations like
- If there is current evidence to refute what the article says, you should have no problem providing refs. -Roxy, the dog. wooF 18:20, 18 February 2019 (UTC)
- Also - I didn't cherry pick - those are just about the only places where CBT is mentioned in the article. ☕ Antiqueight chatter 18:18, 18 February 2019 (UTC)
Cochrane reviews are cited by latest publication date throughout Wikipedia in accordance with convention. If you go to Wiley's landing page there's a "cite this publication" button which you may find informative. We go by published RS, when and if it changes we shall change. Not before. Until then what we have is good. I shall not respond further unless you produce some new WP:MEDRS, as this exchange has degenerated into borderline trolling on your part. Alexbrn (talk) 13:37, 21 February 2019 (UTC)
- Wikipdia's conventions (foolish or wise) don't make that review any more recent. You're the one who described the 2014 Larun review as "a recent Cochrane systematic review - which is about the strongest possible medical source" even though the review itself includes a note from the Editor in Chief of Cochrane which contradicts your claim (which to me implies that you have not read the work you are citing). As a general point for how to live life ethically, and avoid promoting misinformation and prejudice, it is important to read the work one wishes to cite in support of ones claims. You may see this as 'trolling' (given your past behaviour, maybe I should not be surprised by that) but it is actually just concern about the harm being done to those suffering from a stigmatised health condition by people who don't seem to feel that they have a responsibility to examine the validity of the claims they make, or apologise for making misleading claims. Rainywednesday (talk) 14:24, 21 February 2019 (UTC)
False tag of this Talk page
A tag generates this text now:
This is a Wikipedia user talk page. This is not an encyclopedia article or the talk page for an encyclopedia article.
It is false.
-》 Shall we fix the tag? Zezen (talk) 08:06, 18 March 2019 (UTC)
 Done. Alexbrn (talk) 08:23, 18 March 2019 (UTC)
Done. Alexbrn (talk) 08:23, 18 March 2019 (UTC)
Chronotropic intolerance
I just added response to cardiopulmonary exercise test to the list of autonomic abnormalities based on this new meta-study: https://www.frontiersin.org/articles/10.3389/fped.2019.00082/full However, I wanted to ask about this language: "however, these findings have been contradictory." Is that true of all of the findings listed in the sentence? For example, to my knowledge there has not been contradictory findings re: response to CPET. On the contrary, these have been consistent and regardless, this study pooled the average findings of all available studies (https://www.frontiersin.org/files/Articles/420806/fped-07-00082-HTML/image_m/fped-07-00082-t001.jpg). Can't blunted HR response be considered a consistent finding? And can we separate the autonomic nervous system findings that are "contradictory" from the ones that are consistent? Would love any suggestions re: how to do this. Thanks! — Preceding unsigned comment added by Amy2890 (talk • contribs) 15:46, 12 April 2019 (UTC)
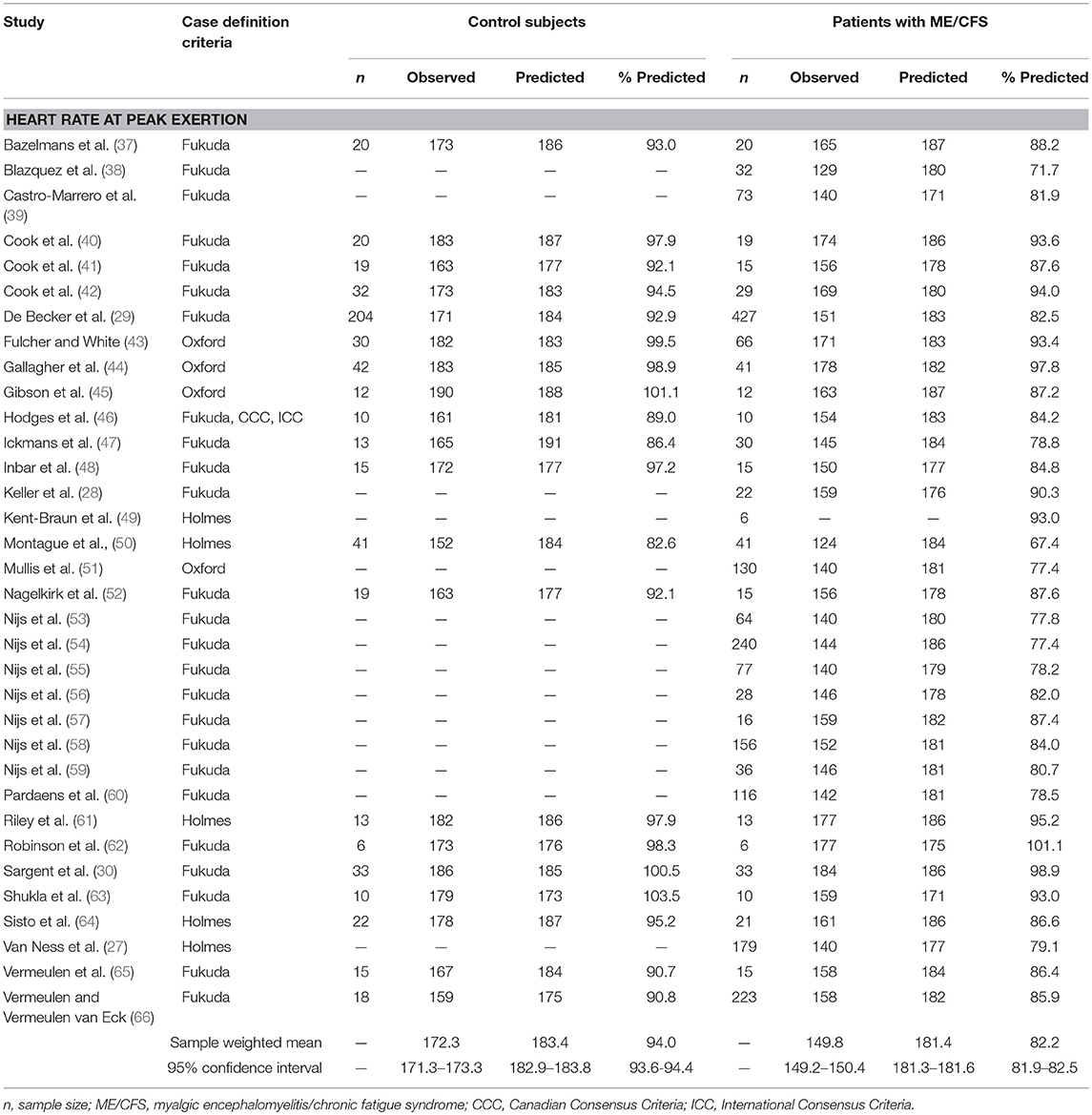{kind=link}
- Frontiers journals are generally not reputable sources for anything non-trivial. Is this covered in better sources? Alexbrn (talk) 15:54, 12 April 2019 (UTC)
I mean...it's a table incorporating 24 studies with an average. It's incredibly simple and easy for anyone to reproduce. All you need is a calculator to check the math. It is the only meta-study of these 24 studies that I am aware of. The sources are the 24 studies. I don't think the journal should matter in a case like this when the results are self-evident (it's not an experiment). I think that it is self-evident should make it trivial Amy2890 (talk) 20:03, 12 April 2019 (UTC)
Weird maths
It contradicts itself:
... people with the condition vary from 7 to 3,000 per 100,000 adults.[7][8] ... most commonly affects people between 40 and 60 years of age.[1][17] Up to 1 in 50 children are estimated to have CFS,...
So from 0 to 3% adults vs 2% children, presumably >5% in adolescents yet most common in a subset of adults?
Maths stinks. Zezen (talk) 20:19, 28 July 2019 (UTC)
Time to Change Page Name to Myalgic Encephalomyelitis
Most researchers have dropped CFS except for historic reasons. The condition is rarely referred to as CFS or CFS/ME nowadays and is normally referred to as ME or ME/CFS.
This has always been a contentious issue. There was an editor vote, perhaps 10 years ago, when ME was supplanting CFS amongst researchers and became the normal term for them to use but ME was rejected as the primary name because it wasn't widely used in the USA amongst medical professionals. As Wikipedia is evidence-based, the evidence is that medical literature is now more in line with patient literature with ME/CFS being the dominant name for the former and ME for the later.
Evidence: I would refer readers to a standard literature search. Examples of use by major research groups:
Centre for Disease Control (CDC) - https://www.cdc.gov/me-cfs/index.html
Harvard - http://endmecfs.mgh.harvard.edu/
Open Medicine Foundation - https://www.omf.ngo/what-is-mecfs/
My second argument is that most patients refer to the illness as ME, rather than CFS (I have not been able to find any CFS charities with Google, I know there used to be one in the USA though). The number of patients with the condition far outweigh the number of outdated health professionals who use the term CFS (mainly out of ignorance). Surely Wikipedia should reflect modern usage by the majority of English speakers and not just a subset of health professionals?
Thirdly, the various diagnostic criteria of ME are far more specific than those for CFS. ME not only represents the primary subset of the CFS population (at least half the CFS population) but is also a more homogenous group. Naturally, this makes it better for research (hence it's predominate use there) but I would also argue that this makes it a better default term for Wikipedia. I have not won this argument on Wikipedia in the past but vague definitions like CFS - either American or British CFS - are confusing and unprofessional and are not what people are looking for. When people (i.e. the users of Wikipedia) look at a disease they expect something well defined and clearly delineated. No iteration of CFS satisfies this but ME does. It is much much easier for people to understand this particular story from the point of view of ME as a foundation and then CFS as a syndrome which includes ME and similar conditions which overlap with it in key areas. I don't think anyone can argue that CFS is a condition in and of itself (there is no evidence to support this) but it is easier to make that case for ME (and increasingly so). Either ME should be explained first (providing a foundation) with CFS second or it should be separated completely from CFS. — Preceding unsigned comment added by Jklsc (talk • contribs) 10:24, 8 September 2019 (UTC)
- There has never been consensus for such a move, despite several discussions over the years. I refer to the archives of the talk pages. One of the (several) issues that actual evidence of encephalomyelitis has never been consistently found. JFW | T@lk 21:28, 8 September 2019 (UTC)
- The English speaking world has moved on since the consensus on the talk page discussions about the name in this article. Looking at the terminology of major national health organizations researching the illness I found:
- CDC now uses Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) as the name.[42]
- Health Council of the Netherlands is using ME/CFS.[45]
- Australia’s National Health and Medical Research Council uses Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS).[46]
- Canadian Institutes of Health Research uses ME/CFS.[47]
- It is very apparent that it is well past time the name of this article should be changed to Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) Ward20 (talk) 05:28, 22 September 2019 (UTC)
- I just don't see how a name change can be justified given the overwhelming disparity in the prevalence of "chronic fatigue syndrome" vs "myalgic encephalomyelitis" in eg search results. I acknowledge that you've hand-picked the some organizations who use your preferred nomenclature, but anyone is free to see via Google search that the majority of organizations, news outlets, etc, use CFS, and the disparity is striking. Given that this is the case, I'm just not seeing the reason for a name change. For what it's worth, I want to note: I get the sense that individuals who suffer from this condition want a name change because ME sounds more "medico-scientific," and while I freely admit that I personally think this is misleading (since there is no unambiguous evidence of an actual "encephalomyelitis," instead this is a suite of symptoms where unambiguous underlying pathophysiology has not yet been identified), I nevertheless think editors should be vigilant and stick to best practices; if the overwhelming majority of organizations like the ones you list used ME, I would gladly agree with a name change (despite my personal opinions). Global Cerebral Ischemia (talk) 13:26, 22 September 2019 (UTC)
- It is very apparent that it is well past time the name of this article should be changed to Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) Ward20 (talk) 05:28, 22 September 2019 (UTC)
- But it isn’t encephalomyelitis, and so it shouldn’t use that name. Roxy, the dog. wooF 13:49, 22 September 2019 (UTC)
- Yeah, I think the use of that term is so bizarre since there is no actual encephalomyelitis present. It speaks to something fishy going on with patient advocacy groups. Not only is there not a single thing in our article about encephalomyelitis per se, I'm not even aware of any wide *claim* that this is even a feature of this syndrome. Global Cerebral Ischemia (talk) 18:58, 22 September 2019 (UTC)
- Whether there is any encephalomyelitis present or not, has no influence what so ever on what this article should be called. Neither does wanting it to sound more scientific. If reliable sources use the term, then it is a valid name. We as Wiki editors are not here to do original research, we are here to collate sources into a tertiary encyclopedia. The CDC, NICE etc are all (very) valid sources for information; they aren't "patient advocacy groups". As shown by the Jklsc above, they use ME/CFS.
- Referring to WP:TITLE:
Generally, article titles are based on what the subject is called in reliable sources. When this offers multiple possibilities, editors choose among them by considering several principles: the ideal article title precisely identifies the subject; it is short, natural, distinguishable and recognizable; and resembles titles for similar articles.
- Having said that, the most recognisable title supported by reliable sources is Chronic fatigue syndrome. Having "Myalgic encephalomyelitis/chronic fatigue syndrome" would be needlessly long. At the moment it seems as though these are two different names for the same condition rather than being treated as a single, combined name (although I might be wrong). The current introduction bolds both, which is Wiki's way of showing that there are two valid names for this condition: others are also given in the infobox. So unless there is clear evidence of ME taking over from CFS or ME/CFS, then the current title satisfies the rules of article titles (without relying on irrelevant arguments about what we ourselves think the condition should or shouldn't be called). Gaia Octavia Agrippa Talk 00:28, 23 September 2019 (UTC)
- For the record, I essentially agree with this. Just to clarify, I don't want my comments to be misinterpreted or misconstrued. While articles must have NPOV, there is no requirement for editors to be neutral in discussions like this. I think my own POV is pretty clear. Nevertheless, as stated in my original comment, I would gladly support a name change if it was warranted, regardless of my own opinions about the strict validity of the terminology per se. Global Cerebral Ischemia (talk) 04:09, 23 September 2019 (UTC)
- Yeah, I think the use of that term is so bizarre since there is no actual encephalomyelitis present. It speaks to something fishy going on with patient advocacy groups. Not only is there not a single thing in our article about encephalomyelitis per se, I'm not even aware of any wide *claim* that this is even a feature of this syndrome. Global Cerebral Ischemia (talk) 18:58, 22 September 2019 (UTC)
Cochrane Exercise therapy review conclusions
The following discussion is closed. Please do not modify it. Subsequent comments should be made on the appropriate discussion page. No further edits should be made to this discussion.
I'd like to note that the conclusions of the Cochrane exercise therapy review (Larun et al 2019 and previous versions) has been subject to several controversies. The first relating to this Wikipedia page is back in 2016 where DocJames added an edit which was misleading, stating "Exercise does not make people worse" when in fact the review stated there was a lack of evidence to form a conclusion. This was subject to several edits and a RfC where a compromise was reached with "no evidence of serious adverse effects was found; however data was insufficient to form a conclusion." Then on September 22nd 2019, ignoring this dispute/discussion, DocJames changed it to: "Exercise therapy is generally beneficial with no evidence that it worsens symptoms". leaving out the bit where there was insufficient evidence. Recently, the article itself has been under review from late 2018, since former Cochrane editor in Chief David Tovey considered that it did not meet Cochrane standards. Some of David Tovey's correspondence with the authors can be accessed via the eInsynn FOI system: https://einnsyn.no/saksmappe?id=http%3A%2F%2Fdata.einnsyn.no%2Fnoark4%2FSaksmappe--983744516--10566--2017 Initially the authors and David Tovey did not seem to be able to compromise, with David Tovey suggesting the Authors withdraw the article. The review of the article seemed to take a long time, being published months after it was promised, with revisions ultimately being published on the 2nd of October 2019.
I would specifically draw attention to the correspondence on 29th of May where David Tovey suggests the following: {{The basis is the important presentation of the absolute results for fatigue at the end of treatment: SMD -0.66, 95% CI -1.01 to -0.31, 7 studies, 840 participants, low certainty evidence, re-expressed MD -3.4, 95% CI -5.3 to -1.6, scale 0 to 33}} Alte Fretheim countered with: {{I proposed a compromise: We simply grade the evidence for this outcome as Low-moderate. The authors have accepted to use the term “may” (usually indicating low certainty evidence) when describing the certainty of the evidence, rather than the term “probably” (usually indicating moderate certainty). They have also accepted not to use any categorization of the effect size. The integrity of our researchers cannot be stretched much more than this. }}
Yet the wording "probably" has remained in the article, reflecting a higher certainty of evidence than was accepted by David Tovey. Hence I urge strong caution to those attempting to overstate the evidence higher than low-moderate certainty. Arch (talk) 10:41, 4 October 2019 (UTC)
- Not sure what the point of this is. We summarize the best sources and if they change, our content follows. People can have legitimate disagreements about how to summarize content - throwing around words like "misleading" doesn't help and is inappropriate for an article Talk page. Alexbrn (talk) 10:46, 4 October 2019 (UTC)
- Alexbrn, how do you define "misleading"? Do you not consider the statement "exercise does not make people worse" to be misleading when the cited reference stated with respect to adverse effects, "but sparse data made it impossible for review authors to draw conclusions" Arch (talk) 10:58, 4 October 2019 (UTC)
Error in Talk:Chronic fatigue syndrome/Archive 4
I want to correct this error in the above. The talk states in the first paragraph:
"The Cause of Chronic Fatigue Syndrome; Light at the End of the Tunnel" Author David Eather. ISBN 0646389025 David is a CFS sufferer who 'discovered' a treatment for his form of CFS. He interested academics and they worked out the biochemical processes involved. He then self-published the book himself in 2000 but is now out of print? As several have expressed a passing interest I have prepared this summary only."
I am David Eather, who wrote this book. My email and witnessed scans of the original documents are available on request. I can state that I alone worked out the biochemical process involved. I had support from 2 general practitioners who lent me their textbooks and answered my endless stupid questions, but I did the rest.
The original purpose of universities was research. Teaching was just a beneficial side effect. It burns my ass that the specialists who were tenured at universities and already paid to research, had no interest in looking at anything about CFS without additional funding. I spoke at some length to DR Neil McGregor from the Newcastle team. I told him directly that the Amino Acid Methionine treatment was a reasonably effective antidote/preventative to a hangover. A proofreader and one of the general practitioners had posed this question about hangovers to me previously, and after consideration, I gave them the answer "yes, it would". McGregor asked me if the Newcastle team's Amino Acid Mixtures would also work for a hangover. I told him, "Yes, of course. Since CFS and hangovers were both aldehyde reactions, anything that worked for CFS would work on a hangover." Less than 2 years later McGregor at el released a product to prevent/cure hangovers called "Alcodol" which had been tested at QUT and shown to be effective. This treatment is a tweaked formula as used by the Newcastle group. Thus, they had their own experimentally backed evidence of the nature of CFS, but rather than research into CFS, they put their efforts into creating a commercial product for an apparently unrelated illness. Before I bought up the subject of treating hangovers with a CFS treatment, none of the Newcastle team had made any investigations down this line.
I stopped my work on CFS for two reasons. Firstly it appeared counterproductive. Researchers are reluctant to put their efforts into confirming or disproving a hypothesis put forward by a layperson. Secondly, I had just spent my superannuation perusing an illness only to watch people who should have been interested, compassionate, better, seemingly turn hard-won information into a grubby cash grab. I was gutted and exhausted.
- We dont edit archives. -Roxy, the PROD. . wooF 11:02, 15 January 2020 (UTC)
If you don't edit archives then at least add a note pointing out errors that you have been informed of. — Preceding unsigned comment added by 58.96.14.19 (talk) 01:00, 16 January 2020 (UTC)
'PACE trial' edit [48]
Using this space to park an edit by Starchify that is misplaced. The PACE trial was about proving CBT and GET effective. Also, blogs and letters are not sufficient references for WP:MEDRS.
The study that popularised Pacing, commonly referred to as the 'PACE trial', has been a cause for much controversy amongst both patients and practitioners, so much so that it even caused the National Institutes of Health (NIH) to recommend the Oxford criteria, which is used to diagnose Chronic fatigue syndrome, and which was used by the PACE trial, be retired[1]. Other criticisms of the study include changes in criteria of how patients' impairment from CFS was changed part way through the study[2], subjectivity within the study's measures[3], apparent conflicts of interest[4], lack of informed consent[4], possible influencing of patients' self-reported outcomes within the study[5], and possible undisclosed side effects of the study[6].
Ward20 (talk) 03:53, 23 May 2020 (UTC)
What symptoms should we list in the lead?
The lead is to be a summary, thus IMO listing >15 possible symptoms "Other symptoms may include muscle pain, joint pain without swelling or redness, muscle weakness, shortness of breath, irregular heartbeat, headache, tender lymph nodes in the neck or armpits, recurring sore throat, digestive issues, chills or night sweats, or sensitivities to foods, odors, lights, chemicals, or noise." is excessive.
Can we trim it down to like 8 maybe such as "Other symptoms may include muscle and joint pain, headaches, tender lymph nodes, recurring sore throat, digestive issues, night sweats, or sensitivities to foods, smells, or lights." Doc James (talk · contribs · email) 14:34, 21 May 2020 (UTC)
- There are 5 core symptoms, with either cognitive dysfunction and orthostatic intolerance required (doesn't have to be both but is often is both). I have just noticed there is a 4 page IOM report brief, we would be best using those symptoms, although with post-exertional malaise first since it's become the hallmark symptom. The CDC Core symptoms section used the same ones. I suggest using the same order but simplifying the medical terms:
- "The disease chronic fatigue syndrome is characterized by profound fatigue, difficulties with thinking and memory, sleep problems, autonomic manifestations, pain, and other symptoms that are made worse by exertion of any sort."
- I think "This disease is characterized by profound fatigue, cognitive dysfunction, sleep abnormalities, dizziness or other problems when sitting or standing, pain, and other symptoms that are made worse by exertion of any sort."[7]: 1
- Beyond that of course are common optional symptoms including sore throat, painful or swollen lymph nodes, endocrine symptoms etc. Amousey (talk) 18:04, 21 May 2020 (UTC)
- With sensitivities, when they are mentioned they need to continue to include light and chemical sensitivity. Similarly, chills and night sweats are mentioned together - part of the "flu-like" symptoms caused by the endocrine system and not to be confused with menopause sweats. I agree that 15 symptoms is too many to list at once, so using "complex" and refering to multiple body systems at the start helps clarify that. I'm happy to work out a table layout if this makes it more readable. Amousey (talk) 18:16, 21 May 2020 (UTC)
- I agree with Doc James. Irregular heartbeat is although a common symptom, however, a person with ME/CFS may not easily detect it and I have not seen any studies that state it causes widespread difficulties. The description "without swelling or redness" is diagnostic but not terribly impactful. "In the neck or armpits" is likewise too detailed. "Muscle weakness is disputable because some studies have shown only a neurological perception of muscle weakness. I haven't noticed good studies on "shortness of breath" to determine prevalence or pathology. Ward20 (talk) 22:54, 21 May 2020 (UTC)
- Without joint swelling or redness is essential to keep in because it rules out the majority of alternative causes of joint pain - they've chosen to keep that detail on the short list because of of significance. I think with the lymph nodes, many different criteria have mentioned that without specifing which lymph nodes so I am fine to leave it out. It would be wrong to leave out irregular heartbeat however. It made the short list of symptoms after they read thousands of research papers.
- User:Ward20 I would expect it be in large studies not case studies with only a handful of patients. See PMC6703845, the list of symptoms in the Canadian Consensus Criteria and International Consensus Criteria too. It needs to stay. Heart palpitations are in the this primer. Also bear in mind what the T in POTS stands for... the deaths from heart related problems are one of the three leading causes of deaths in this disease. It's clearly important. Amousey (talk) 23:21, 21 May 2020 (UTC)
- I agree "without swelling or redness" should be part of the sign and symptoms diagnostic discussion section, but I believe it is too much detail in the lead where the article is summarizing the symptoms. Irregular heartbeat is not the same as heart failure described in Jason's paper. He hypothesizes several different mechanisms as possible contributors to the heart failure such as; "decreases in circulating blood volume, lower cardiac output, as well as sympathetic transmission to the heart". That said, I would not have a issue keeping it in due to the fact it's mentioned so often in so many secondary sources.Ward20 (talk) 00:11, 22 May 2020 (UTC)
- Let's just keep the main 5, and take out/move the "other symptoms" paragraph from the lead section, and put after the main 5 something like:
- I agree "without swelling or redness" should be part of the sign and symptoms diagnostic discussion section, but I believe it is too much detail in the lead where the article is summarizing the symptoms. Irregular heartbeat is not the same as heart failure described in Jason's paper. He hypothesizes several different mechanisms as possible contributors to the heart failure such as; "decreases in circulating blood volume, lower cardiac output, as well as sympathetic transmission to the heart". That said, I would not have a issue keeping it in due to the fact it's mentioned so often in so many secondary sources.Ward20 (talk) 00:11, 22 May 2020 (UTC)
"although many [#Signs_and_Symptoms other symptoms] typically occur, which affecting multiple body systems".
- They can click the link to jump lower if interested. Amousey (talk) 00:36, 22 May 2020 (UTC)
- I think that is an excellent idea. Working on it. Ward20 (talk) 01:57, 22 May 2020 (UTC)
- The lead is getting repetitive. We say "multisystem" and "affecting numerous body systems". We do not need both in the same paragraph of the lead. Doc James (talk · contribs · email) 13:28, 22 May 2020 (UTC)
- Repetitive terms in lead: "multisystem" and "affecting numerous body systems", Fixed now, correct? Ward20 (talk) 01:49, 24 May 2020 (UTC)
- The lead is getting repetitive. We say "multisystem" and "affecting numerous body systems". We do not need both in the same paragraph of the lead. Doc James (talk · contribs · email) 13:28, 22 May 2020 (UTC)
- I think that is an excellent idea. Working on it. Ward20 (talk) 01:57, 22 May 2020 (UTC)
- They can click the link to jump lower if interested. Amousey (talk) 00:36, 22 May 2020 (UTC)
Short description
This is out of date. It currently says:
- Medical condition involving extreme fatigue among other symptoms
I think it should say
- Complex disease involving multiple body systems that results in exertion intolerance, extreme fatigue and other symptoms.
"Complex" and "multiple body systems" coming from the CDC description, the use of exertion intolerance from the Systematic Exertion intolerance Disease name. Amousey (talk) 18:11, 21 May 2020 (UTC)
- Appears like an improvement to me. Ward20 (talk) 22:57, 21 May 2020 (UTC)
- Were does the article say "Medical condition involving extreme fatigue among other symptoms" Doc James (talk · contribs · email) 09:54, 22 May 2020 (UTC)
- User:Doc James In the short description template, the single line above the table. Amousey (talk) 10:38, 22 May 2020 (UTC)
- Were does the article say "Medical condition involving extreme fatigue among other symptoms" Doc James (talk · contribs · email) 09:54, 22 May 2020 (UTC)
- Amousey, no thanks - "complex disease" incorporates a number of unproven assumptions. Guy (help!) 10:48, 22 May 2020 (UTC)
- Guy it's the primary conclusion of the IOM report, see bottom of page 5. The CDC also consistently uses the term "complex" and the World Health Organization classes it under Diseases, and excludes it from "General signs and symptoms". The name SEID is Systemic Exertion Intolerance Disease Amousey (talk) 11:20, 22 May 2020 (UTC)
- Amousey, feel free to show the pathology that shows this is a disease rather than a condition or disorder. Guy (help!) 12:46, 22 May 2020 (UTC)
- I know there's a policy about "Not A Forum," but chances are you won't be hearing from me much. I just got to a point where I had to mention something about statements like this. I'm not completely up on WP policy to the point of which one supersedes the other, but this struck me as something caught somewhere in the truth/verifiability vortex. You're asking him to 'show pathology' when what he's doing is citing verifiable sources that meet MEDRS. Confusing at best. Moreover, and I don't mean to pick on Guy here, but further up the page he laments the current cluster of edits as a manifestation of an activist agenda. What does that have to do with the reliability of sources such as the CDC and the Institute of Medicine? It sort of reminds me of a few years ago when a now self-banished editor vetoed an edit from a NIH publication because he claimed it didn't meet MEDRS. It was published in the Annals of Internal Medicine (there were editorials alongside actual studies, but the edit was about one of the actual studies) but didn't meet MEDRS? It's sort of difficult to accept that there's only been a one-way agenda to attempt to keep the content of this article neutral over the years. But when it comes to this topic there can be a real lack of common sense, on both sides, but...geez. Guy, you're now claiming that the changes we've seen in this area over the past few years have anything to do with activist lobbying of the CDC? Seriously? They consistently drew criticism from patient lobbies for decades, but now all of a sudden they're going in a direction you find unscientific/inaccurate because of activist pressure? If you haven't been paying attention, it's nearly five years since qualified professionals started to take a good, long, hard look at PACE (perhaps because, although it would constitute OR here, there were, apparently, people who wondered how you treat an intolerance to exertion resulting in relapse, with graduated exercise). That, I believe you'll find, is a large part of why this is happening, with the other being the large volume of research published in recent years that conflicts with prior guidance about ME/CFS. Look, the CFS article you created on RationalWiki is quite revealing: you're hardly alone in this, but for a lot of medical science, CFS is characterized mostly by what we know about patient activism, but little about the illness itself. Now we don't have convincing pathology or a number of other essential components here, yet the IOM said we need to classify this as a disease. The CDC has adopted their criteria and apparently many of the recommendations. You can't dismiss that because it conflicts with your previously held views, but you knew that. Did you ever consider that the activists might have been correct? Okay, enough, I apologize for the soapboxing, but I've followed this article for over a decade and read the Talk archives, and in spite of whatever stupidity or pigheadedness from this or that 'activist,' it's simply maddening at times. I know this is against policy, I won't do it again, I promise, apologies. But I had to get that off my chest. NeurastheniaMilkshake (talk) 04:43, 23 May 2020 (UTC)
- Amousey, feel free to show the pathology that shows this is a disease rather than a condition or disorder. Guy (help!) 12:46, 22 May 2020 (UTC)
- Guy it's the primary conclusion of the IOM report, see bottom of page 5. The CDC also consistently uses the term "complex" and the World Health Organization classes it under Diseases, and excludes it from "General signs and symptoms". The name SEID is Systemic Exertion Intolerance Disease Amousey (talk) 11:20, 22 May 2020 (UTC)
Thanks for your comments NeurastheniaMilkshake. Guy sources for the disease: IOM report including the SEID name - Systemic Exercise Intolerance Disease, the WHO classification [https://icd.who.int/browse10/2016/en#/G93 — Preceding unsigned comment added by Amousey (talk • contribs) 15:51, 24 May 2020 (UTC)
Free 1hr CPD module
I had this flagged up to me recently, 1hr free online training on CFS, with CPD credits
I ran through it the other day and noticed some very good referencing and explanations. I thought it might interest you. If you don't assess patients that option can be left blank. Amousey (talk) 00:07, 22 May 2020 (UTC)
- We do not generally link CME links within Wikipedia articles. Doc James (talk · contribs · email) 09:49, 22 May 2020 (UTC)
- I wasn't planning to, simply posting here for editors interested in some free training resources. I presume some professionals are editors here. User:Doc James Amousey (talk) 16:00, 24 May 2020 (UTC)
- We do not generally link CME links within Wikipedia articles. Doc James (talk · contribs · email) 09:49, 22 May 2020 (UTC)
Risk factors
User:Ward20 I can see you editing this at the moment, so posting risk factors here rather than risking an edit conflict.
- Female gender
- Viruses (Epstein-Barr, Ross River Virus, etc)
- Nonviral infections[8][9][10]: 20
- Genetic predisposition[11][12]: 1–2
- Major injury or anaesthetic[11][12]: 1–2
- Bodily response to severe stress[11][12]: 1–2 [10]: 21
- Exposure to toxins[12]: 1–2 [13]
- Vaccinations[12]: 1–2
Is it worth mentioning SARS or flu with the other viruses (SARS CFS outbreak in Hong Kong - Lam 2009)? Amousey (talk) 23:32, 22 May 2020 (UTC)
- OK thank, I have a bit more to do there to find reliable sources for some material cited to the CDC where the page was removed. Then I will come back here and write when I am done for the day. All good points on the risk factors but make sure that the information can be cited from well known journal and is a review and just not a primary study. Makes it much easier to justify the material. Ward20 (talk) 23:51, 22 May 2020 (UTC)
- Done with risk factors for now. Concering the recent edits: I believe ("brain fog") is too detailed, and too much jargon for the lead. biological, genetic, infectious, and psychological was better wording than what is there now, as it was concise and covered all the hypotheses, physical or psychological stress affecting body chemistry is the same as biological but just more words. The Suggested diagnostic tools section is nice but these articles don't normally present this type of information. See WP:NOTMANUAL. Ward20 (talk) 01:23, 23 May 2020 (UTC)
- I've updated the wording User:Ward20 and added references. It can also be any virus as a risk factor. The CDC's physical or psychological stress affecting body chemistry is different to biological but an example of biological so I guess there's some duplication, it's referring to physical trauma (major accident, surgery) or overwhelming stress (new CDC wording that replaces psychological) - this is coming from the CDC page. The IOM report only says "The cause of ME/CFS remains unknown, although in many cases, symptoms may have been triggered by an infection or other prodromal event, such as "immunization, anesthetics, physical trauma, exposure to environmental pollutants, chemicals and heavy metals, and rarely blood transfusions" (Carruthers and van de Sande, 2005, p. 1)." p1. . Any of the primers or clinician consensus documents in the external sources also make good secondary sources. [https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6370741/ Chu 2019 is a major study of onset factors. Amousey (talk) 19:33, 24 May 2020 (UTC)
Should Risk factors be a subset under Epidemiology?
Otherwise there is going to be a lot of duplication of material. There already is duplication since the sections are now separate. Ward20 (talk) 07:02, 25 May 2020 (UTC)
References
- ^ National Institutes of Health (US) (Dec 9, 2014), NIH Pathways to Prevention Workshop: Advancing the Research on Myalgic Encephalomyelitis/ Chronic Fatigue Syndrome https://prevention.nih.gov/sites/default/files/documents/programs/mecfs/ODP-P2P-MECFS-FinalReport.pdf
- ^ White, P. D.; Goldsmith, K. A.; Johnson, A. L.; Potts, L.; Walwyn, R.; DeCesare, J. C.; Baber, H. L.; Burgess, M.; Clark, L. V.; Cox, D. L.; Bavinton, J. (2011-03-05). "Comparison of adaptive pacing therapy, cognitive behaviour therapy, graded exercise therapy, and specialist medical care for chronic fatigue syndrome (PACE): a randomised trial". The Lancet. 377 (9768): 823–836. doi:10.1016/S0140-6736(11)60096-2. ISSN 0140-6736. PMID 21334061.
- ^ Torjesen, Ingrid (2015-01-14). "Tackling fears about exercise is important for ME treatment, analysis indicates". BMJ. 350. doi:10.1136/bmj.h227. ISSN 1756-1833. PMID 25589087.
- ^ a b "An open letter to The Lancet, again". www.virology.ws. Retrieved 2020-05-23.
- ^ "TRIAL BY ERROR: The Troubling Case of the PACE Chronic Fatigue Syndrome Study". www.virology.ws. Retrieved 2020-05-23.
- ^ "Our Illness Management Report on CBT, GET and Pacing calls for major changes to therapies offered for ME/CFS | 29 May 2015". ME Association. 2015-05-28. Retrieved 2020-05-23.
- ^ https://www.nap.edu/resource/19012/MECFS_ReportBrief.pdf
- ^ https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1524744
- ^ https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1569956/
- ^ a b https://www.cdc.gov/grand-rounds/pp/2016/20160216-presentation-chronic-fatigue-H.pdf
- ^ a b c https://www.cdc.gov/me-cfs/about/possible-causes.html
- ^ a b c d e Cite error: The named reference
ICC2011primerwas invoked but never defined (see the help page). - ^ https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6370741/
This text failed verification
Onset was listed as "Any age" with this as the reference https://www.cdc.gov/me-cfs/index.html
I am not seeing that this page supports? Doc James (talk · contribs · email) 13:34, 22 May 2020 (UTC)
- I will add the reference. User:Doc James "ME/CFS is often thought of as a problem in adults, but children (both adolescents and younger children) can also get ME/CFS." CDC - children. Previously stating only ages 40-60 I felt was misleading, given the number of pediatric primers and the fact that I have never seen any reference to a maximum age or that pensioners can't get it. There are some references showing it is the main source of school absence. Amousey (talk) 16:04, 24 May 2020 (UTC)
- That is not "any age". Best to list the most common age in the infobox as that is what the line indicates. Doc James (talk · contribs · email) 05:32, 25 May 2020 (UTC)
- Not disputing what should or shouldn't go in the infobox, but Risk Factors does state "any age" based on the CDC epidemiology page that states "anyone can get ME/CFS".[49] Does that support "any age" in Risk factors in your opinion? Ward20 (talk) 06:53, 25 May 2020 (UTC)
- Yes agree "but can occur at other ages including in children" is supported. Moved next to the usual age in the lead. Doc James (talk · contribs · email) 08:52, 25 May 2020 (UTC)
- Not disputing what should or shouldn't go in the infobox, but Risk Factors does state "any age" based on the CDC epidemiology page that states "anyone can get ME/CFS".[49] Does that support "any age" in Risk factors in your opinion? Ward20 (talk) 06:53, 25 May 2020 (UTC)
- That is not "any age". Best to list the most common age in the infobox as that is what the line indicates. Doc James (talk · contribs · email) 05:32, 25 May 2020 (UTC)
Cochrane (2019) embargoed
The ref named Lar2019 is embargoed - see here, not released until October 2020, but it's used in a number of places even with a direct quote. I assume this is a mistake and the reference refers to one of the previous versions of this review. If someone could figure out which that would be helpful. At present, a rewrite is ongoing due to it failing to meet the Cochrane requirements - so we can't rely on its accuracy as we normally would. I think we should look to other systematic reviews on this. The latest amendment was May 21, 2020. It now points to this update stating "...It now places more emphasis on the limited applicability of the evidence to definitions of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) used in the included studies, the long-term effects of exercise on symptoms of fatigue, and acknowledges the limitations of the evidence about harms that may occur." The May 21st Cochrane Review now states:
"Exercise therapy may make little or no difference to fatigue at end of treatment (MD 0.20, 95% Cl -1.49to 1.89; 1 study, 298 participants; low-certainty evidence), or at long-term follow-up (SMD 0.07,95% Cl -0.13 to 0.28; 2 studies, 351 participants; moderate-certainty evidence).
We are uncertain about the risk of serious adverse reactions because the certainty of the evidence is very low (RR 0.67,95% Cl 0.11 to 3.96; 1 study, 321 participants).
The available evidence suggests that there may be little or no difference between exercise therapy and CBT in physical functioning or sleep (low-certainty evidence) and probably little or no difference in the effect on depression (moderate-certainty evidence). We are uncertain if exercise therapy compared to CBT improves quality of life or reduces pain because the evidence is of very low certainty."
— Preceding unsigned comment added by Amousey (talk • contribs) 00:30, 22 May 2020 (UTC)
Taking this into account, I don't think graded exercise therapy should be a treatment in the summary box - and the CDC website confirms it isn't an approved treatment. The CDC states[1] "There is no cure or approved treatment for myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). However, some symptoms can be treated or managed." I think perhaps activity management (pacing) should be added based on the CDC info, plus this huge survey conducted for NICE in the UK. In brief the survey showed:
- Graded exercise therapy or GET with CBT made most people worse
- CBT didn't help or worsen most people, and people were more likely to get worse than better with it
- CBT only improved physical health for 16% of patients, but mental health improved for a large number - suggesting this can't be a primary treatment but may be helpful for those with mental health issues in addition to chronic fatigue syndrome (CFS doesn't have any any mental health symptoms itself but as with other Chronic illnesses rates of depression are higher than in healthy people).
- Pacing (ie activity management) has some evidence from many different patient surveys, plus the Consensus pmid 22181560 on it by Goudsmit, Jason and Wallmam (2012). Amousey (talk) 00:02, 22 May 2020 (UTC)
- I think this should be handled with care. I am not sure it requires a substantial change in the lead at this time because appropriate caveats about GET were put in a while ago. When the revised Cochrane review comes out in October and the NICE guidance for CFS/ME comes out in December there should be better guidence about GET. It would be better to work on consensus in GET section first and it will be easier to determine how to describe GET in the lead.
- About Pace. The CDC is recommending it and I just reviewed the NICE Clinical guideline.[50] Although they say at 1.4.2.7 "there is insufficient research evidence on the benefits or harm of pacing", at 1.7.2.3 they do recommend pacing for managing a setback/relapse. So, I agree that Pacing should probably be elevated into the lead as a recommended therapy. The survey designed by a steering group of Forward ME members, implemented by others, and forwared to NICE is interesting, but NICE will have to report on it before the acticle should give it any WP:WEIGHT. Ward20 (talk) 01:27, 22 May 2020 (UTC)
- Agree with User:Ward20, we should wait for these guidelines / reviews to be published. Doc James (talk · contribs · email) 09:52, 22 May 2020 (UTC)
- User:Doc James You agree with User:Ward20 on elevating pacing to the top box, but on not referencing the survey until NICE review it? The NICE guidelines are under review, partly because they rely so heavily on a contested exercise review by Cochrane which Cochrane has updated a number of times since the 2007 guidelines were published - including changing the Conclusions. In the top box, perhaps the wording for treatment could be "symptomatic; pacing is recommended for post-exertional malaise". Source:[2] Amousey (talk) 11:43, 22 May 2020 (UTC)
- We currently say "gradual increase in activity" which I think is fine in the infobox. Doc James (talk · contribs · email) 11:58, 22 May 2020 (UTC)
- What references to you have to support that User:Doc James? I have given substantial references against it. Gradual increases are the definition of graded exercise therapy (GET involves increase in any activity not simply "exercise" - increasing the length of time spent on schoolwork is typical for GET in children). "Activity management" would be ok. CDC does not mention "gradual increase".Amousey (talk) 17:25, 22 May 2020 (UTC)
- I don't think that gradual increase in activity, describes pacing properly. The CDC defines pacing similar to staying within individual limits for mental and physical activity.[51] Ward20 (talk) 19:57, 22 May 2020 (UTC)
- The one source says "Exercise therapy probably has a positive effect on fatigue in adults with CFS compared to usual care or passive therapies."[52]
- The other says "graded exercise therapy suggest benefit for some patients meeting case definitions for CFS"[53]
- Doc James (talk · contribs · email) 09:35, 23 May 2020 (UTC)
- Not saying that graded exercise therapy is not supported by reliable sources or that it should be changed in the article. I'm saying that pacing is a separate strategy that is recommended by CDC and NICE (see above) in order to prevent relapses from exertion. These therapies are not mutually exclusive. A gradual increase in activity is fine if it stays within the energy envelope of an individual so that it does not induce a severe bout of PEM. Since it is recommended by at least the two guidelines I think it should be mentioned in the lead and infobox. The Pacing material in the body needs updating though. Maybe after that there will be a consensus (or not) for wording in the lead. Ward20 (talk) 10:12, 23 May 2020 (UTC)
- What wording do you propose? Would be good to describe pacing therapy in common English. Not sure how to do so. Doc James (talk · contribs · email) 08:01, 24 May 2020 (UTC)
- Not saying that graded exercise therapy is not supported by reliable sources or that it should be changed in the article. I'm saying that pacing is a separate strategy that is recommended by CDC and NICE (see above) in order to prevent relapses from exertion. These therapies are not mutually exclusive. A gradual increase in activity is fine if it stays within the energy envelope of an individual so that it does not induce a severe bout of PEM. Since it is recommended by at least the two guidelines I think it should be mentioned in the lead and infobox. The Pacing material in the body needs updating though. Maybe after that there will be a consensus (or not) for wording in the lead. Ward20 (talk) 10:12, 23 May 2020 (UTC)
- We currently say "gradual increase in activity" which I think is fine in the infobox. Doc James (talk · contribs · email) 11:58, 22 May 2020 (UTC)
- About Pace. The CDC is recommending it and I just reviewed the NICE Clinical guideline.[50] Although they say at 1.4.2.7 "there is insufficient research evidence on the benefits or harm of pacing", at 1.7.2.3 they do recommend pacing for managing a setback/relapse. So, I agree that Pacing should probably be elevated into the lead as a recommended therapy. The survey designed by a steering group of Forward ME members, implemented by others, and forwared to NICE is interesting, but NICE will have to report on it before the acticle should give it any WP:WEIGHT. Ward20 (talk) 01:27, 22 May 2020 (UTC)
(Out) Well I still need to finish the article Pacing section, probably based on the second and third paragraphs of the Treatment PEM section of the CDC page.[54] Avoiding severe PEM during the initial illness onset is very important. ("Prominent risk factors that predict progression are the severity of the symptoms at the time of onset, the standard of early management of the disease,...poor control over the symptoms have been associated with worse outcomes".)[55]
But my thinking for the lead wording is something similar to: Activity management may help avoid worsening of symptoms caused by the exertion of doing routine tasks. Ward20 (talk) 09:54, 24 May 2020 (UTC)
- Simply "pacing (activity management)" added to "symptomatic". Although we could put "symptomatic e.g. pain medication" since the is extensive evidence for that treating the pain symptom only. User:Doc James to avoid confusion with the Adaptive Pacing Therapy that the PACE trial tried and found not effective (see my new section on this). To be honest shocked to see no page on pacing on Wikipedia, despite the huge one in spoon theory (which is a way to understand / explain / use pacing). BTW note the Oct 2019 update from Cochrane about the results having limited relevance to ME/CFS. Amousey (talk) 15:58, 24 May 2020 (UTC)
- Something is wrong with citation ref name=Lar2019. The 2020 version can be accessed,[56] but I don't know which version the article is using so if someone could help... Ward20 (talk) 09:51, 25 May 2020 (UTC)
- Looks like User:Amousey fixed it. Thanks. Ward20 (talk) 01:53, 26 May 2020 (UTC)
- Next time just revert as many times as needed. It was a nightmare to fix. Amousey (talk) 01:58, 26 May 2020 (UTC)
- Yes I found out it was a bugger and couldn't fix it. I wasn't editing anything in that section so I had no idea what to revert and didn't want to take out anyone's hard work. Ward20 (talk) 02:07, 26 May 2020 (UTC)
- Next time just revert as many times as needed. It was a nightmare to fix. Amousey (talk) 01:58, 26 May 2020 (UTC)
References
- ^ https://www.cdc.gov/me-cfs/treatment/index.html
- ^ "Treatment of ME/CFS".
PEM can be addressed by activity management, also called pacing. The goal of pacing is to learn to balance rest and activity to avoid PEM flare-ups, which can be caused by exertion that patients with ME/CFS cannot tolerate. To do this, patients need to find their individual limits for mental and physical activity.
Management and treatments headings
Previously the Exercise therapy heading only referred to GET and not to exercise advice from CDC, and no counseling section was available for counseling that did not involve CBT aimed at a specific model of CFS. Headings have now been added for these factors, and CBT, GET and APT have been moved under therapies since they are not management strategies. Medication used for symptom management and other CDC recommendations may need additional headings. Current structure as below.
- 5 Management
Pacing above refers to activity management pacing, not pacing as a treatment (not APT). Note that non-CBT counseling methods have also been used in CFS as a management strategy. Rintatolimod while not approved should probably have a higher level heading eg in Therapies since there is some evidence, although not for all patients. Isn't there a program now to access it for CFS on compassionate grounds? Amousey (talk) 11:46, 26 May 2020 (UTC)