
Prediabetes
| Prediabetes | |
|---|---|
 | |
| White hexagons in the image represent glucose molecules, which are increased in the lower image. Hyperglycemia is the only major sign of prediabetes. | |
| Specialty | Endocrinology |
| Complications | Diabetic complications |
Prediabetes is a component of metabolic syndrome and is characterized by elevated blood sugar levels that fall below the threshold to diagnose diabetes mellitus. It usually does not cause symptoms but people with prediabetes often have obesity (especially abdominal or visceral obesity), dyslipidemia with high triglycerides and/or low HDL cholesterol, and hypertension.[1] It is also associated with increased risk for cardiovascular disease (CVD). Prediabetes is more accurately considered an early stage of diabetes as health complications associated with type 2 diabetes often occur before the diagnosis of diabetes.
Prediabetes can be diagnosed by measuring hemoglobin A1c, fasting glucose, or glucose tolerance test. Many people may be diagnosed through routine screening tests. The primary treatment approach includes lifestyle changes such as exercise and dietary adjustments. Some medications can be used to reduce the risks associated with prediabetes. There is a high rate of progression to type 2 diabetes but not everyone with prediabetes develops type 2 diabetes.[2] Prediabetes can be a reversible condition with lifestyle changes.
For many people, prediabetes and diabetes are diagnosed through a routine screening at a check-up. The earlier prediabetes is diagnosed, the more likely an intervention will be successful.
Signs and symptoms
[edit]Prediabetes typically has no distinct signs or symptoms except the sole sign of high blood sugar.[3] Patients should monitor for signs and symptoms of type 2 diabetes mellitus such as increased thirst, increased urination, and feeling tired.[4]
Causes
[edit]The cause of prediabetes is multifactorial and is known to have contributions from lifestyle and genetic factors. Ultimately prediabetes occurs when control of insulin and blood glucose in the body becomes abnormal, also known as insulin resistance.[5] Risk factors for developing prediabetes include being overweight or obese, physical inactivity, an unhealthy diet, a family history of diabetes, having a genetic predisposition to prediabetes or diabetes, older age, and women who have a history of gestational diabetes or high birth weight infants (greater than 9 lbs.).[6][7]
The increasing rates of prediabetes and diabetes suggest lifestyle and/or environmental factors that contribute to prediabetes. It remains unclear which dietary components are causative and risk is likely influenced by genetic background.[8] Increasing physical activity and following a healthy diet can reduce the risk of progressing to type 2 diabetes.[6]
Pathophysiology
[edit]Normal glucose homeostasis is controlled by three interrelated processes. These processes include gluconeogenesis (glucose production that occurs in the liver), uptake and utilization of glucose by the peripheral tissues of the body, and insulin secretion by the pancreatic beta islet cells. The presence of glucose in the bloodstream triggers the production and release of insulin from the pancreas' beta islet cells. The main function of insulin is to increase the rate of transport of glucose from the bloodstream into certain cells of the body, such as striated muscles, fibroblasts, and fat cells. It also is necessary for transport of amino acids, glycogen formation in the liver and skeletal muscles, triglyceride formation from glucose, nucleic acid synthesis, and protein synthesis. In individuals with prediabetes, a failure of pancreatic hormone release, failure of targeted tissues to respond to the insulin present or both leads to blood glucose rises to abnormally high levels.[9]
Diagnosis
[edit]Prediabetes can be diagnosed with three different types of blood tests:[10]
- Fasting blood sugar (glucose) level of:
- 110 to 125 mg/dL (6.1 mmol/L to 6.9 mmol/L) – WHO criteria
- 100 to 125 mg/dL (5.6 mmol/L to 6.9 mmol/L) – ADA criteria
- Glucose tolerance test: blood sugar level of 140 to 199 mg/dL (7.8 to 11.0 mM) 2 hours after ingesting a standardized 75 gram glucose solution (WHO and ADA criteria)[10]
- Glycated hemoglobin (HbA1c) between 5.7 and 6.4 percent, i.e. 38.9 and 46.4 mmol/mol[10]
Levels above these limits would justify a diagnosis for diabetes.
Impaired fasting glucose
[edit]Impaired fasting glycemia or impaired fasting glucose (IFG) refers to a condition in which the fasting blood glucose is elevated above what is considered normal levels but is not high enough to be classified as diabetes mellitus. It is considered a pre-diabetic state, associated with insulin resistance and increased risk of cardiovascular pathology, although of lesser risk than impaired glucose tolerance (IGT). IFG sometimes progresses to type 2 diabetes mellitus.[citation needed]
Fasting blood glucose levels are in a continuum within a given population, with higher fasting glucose levels corresponding to a higher risk for complications caused by the high glucose levels. Some patients with impaired fasting glucose also may be diagnosed with impaired glucose tolerance, but many have normal responses to a glucose tolerance test. Fasting glucose is helpful in identifying prediabetes when positive but has a risk of false negatives.[11]
World Health Organization (WHO) criteria for impaired fasting glucose differs from the American Diabetes Association (ADA) criteria, because the normal range of glucose is defined differently by each. Fasting plasma glucose levels 100 mg/dL (5.5 mmol/L) and higher have been shown to increase complication rates significantly, however, WHO opted to keep its upper limit of normal at under 110 mg/dL for fear of causing too many people to be diagnosed as having impaired fasting glucose, whereas the ADA lowered the upper limit of normal to a fasting plasma glucose under 100 mg/dL.[12]
- WHO criteria: fasting plasma glucose level from 6.1 mmol/L (110 mg/dL) to 6.9 mmol/L (125 mg/dL)[13][14]
- ADA criteria: fasting plasma glucose level from 5.6 mmol/L (100 mg/dL) to 6.9 mmol/L (125 mg/dL)[12]
Impaired glucose tolerance
[edit]Impaired glucose tolerance (IGT) is diagnosed with an oral glucose tolerance test. According to the criteria of the World Health Organization and the American Diabetes Association, impaired glucose tolerance is defined as:[13][14]
- two-hour glucose levels of 140 to 199 mg per dL (7.8 to 11.0 mmol/L) on the 75-g oral glucose tolerance test. A patient is said to be under the condition of IGT when he/she has an intermediately raised glucose level after 2 hours, but less than the level that would qualify for type 2 diabetes mellitus. The fasting glucose may be either normal or mildly elevated.
From 10 to 15 percent of adults in the United States have impaired glucose tolerance or impaired fasting glucose.[15]
Hemoglobin A1c
[edit]Hemoglobin A1c is a measure of the percent of red blood cells that are glycated, or have a glucose molecule attached. This can be used as an indicator of blood glucose level over a longer period of time and is often used to diagnose prediabetes as well as diabetes. HbA1c may not accurately represent blood glucose levels and should not be used in certain medical conditions such as iron-deficiency anemia, Vitamin B12 and folate deficiency, pregnancy, hemolytic anemia, an enlarged spleen, and end-stage kidney failure.[5]
Fasting Insulin
[edit]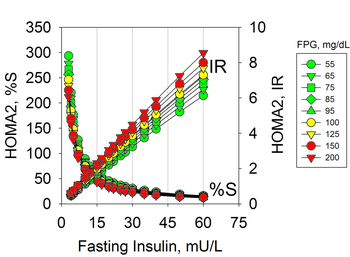
Hyperinsulinemia due to insulin resistance may occur in individuals with normal glucose levels and therefore is not diagnosed with usual tests. Hyperinsulinemia precedes prediabetes and diabetes that are characterized by hyperglycemia.[16] Insulin resistance can be diagnosed by measures of plasma insulin, both fasting or during a glucose tolerance test.[17][18] The use of fasting insulin to identify patients at risk has been proposed, but is currently not commonly used in clinical practice.[19]
The implications of hyperinsulinemia is the risk of comorbidities related to diabetes that may precede changes in blood glucose,[20][21][16] including cardiovascular diseases.[22][23][24]
Screening
[edit]Fasting plasma glucose screening should begin at age 30–45 and be repeated at least every three years. Earlier and more frequent screening should be conducted in at-risk individuals. The risk factors for which are listed below:
- Family history (parent or sibling)
- Dyslipidemia (triglycerides > 200 mg/dL or HDL < 35 mg/dL)
- Overweight or obesity (body mass index > 25 kg/m2)
- History of gestational diabetes or infant born with birth weight greater than 9 lb (4 kg)
- High risk ethnic group (such as of being of African American, Hispanic, Native American, Asian American or Pacific Islander heritage)
- Hypertension (systolic blood pressure >140 mmHg or diastolic blood pressure > 90 mmHg)
- Prior fasting blood glucose > 99 mg/dL
- Known vascular disease
- Markers of insulin resistance (PCOS, acanthosis nigricans)[25][26]
The United States Preventative Services Task Force (USPSTF) recommends adults who are overweight/obese and aged 40–70 years old to get screened during visits to their regular physician. The American Diabetes Association (ADA) recommends normal testing repeated every three years and recommends a larger range of people get tested: anyone over the age of 45 regardless of risk; an adult of any age who is obese or overweight and has one or more risk factors, which includes hypertension, a first degree relative with diabetes, physical inactivity, high risk race/ethnicity, Asian Americans with BMI of ≥23 kg/m2, HDL < 35 mg/dL or TG > 250 mg/dL, women who have delivered child >9 lbs or with gestational diabetes, A1c ≥ 5.7%, impaired fasting glucose (IFG) or impaired glucose tolerance (IGT).[27]
In the UK, NICE guidelines suggest taking action to prevent diabetes for people with a body mass index (BMI) of 30. For people of Black African, African-Caribbean, South Asian and Chinese descent the recommendation to start prevention starts at the BMI of 27,5.[28] A study based on a large sample of people in England suggest even lower BMIs for certain ethnic groups for the start of prevention, for example 24 in South Asian and 21 in Bangladeshi populations.[29][30]
Early detection and management
[edit]Over half the people who are diagnosed with prediabetes eventually develop type 2 diabetes and once diagnosed with prediabetes, people experience a range of emotions: distress and fear; denial and downplay of risks; guilt and self-criticism; and self-compassion. While prediabetes is a reversible condition, it requires diet change and exercise, which may be more difficult for people diagnosed prediabetes because facing the risk of a chronic condition is associated with negative emotions, which further hinder the self-regulation that is required in reversing a prediabetes diagnosis.[31] Still, without taking action, 37% of individuals with prediabetes will develop diabetes in only 4 years, and lifestyle intervention may decrease the percentage of prediabetic patients in whom diabetes develops to 20%.[32] The National Diabetes Prevention Program (DPP) has a Center of Disease Control (CDC)-recognized lifestyle change program that showed prediabetic people following the structured program can cut their risk of developing type 2 diabetes by 58% (71% for people over 60 years old).[33] Considering the possibility to recover from the prediabetic status but also this emotional struggle upon diagnosis, it is encouraged for higher risk patients to get tested early. Having an additional screening option in the dental setting may offset some of the emotional struggle because it is more regularly visited and therefore has the potential to initiate earlier recognition and intervention.[citation needed]
Prevention
[edit]The American College of Endocrinology (ACE) and the American Association of Clinical Endocrinologists (AACE) have developed lifestyle intervention guidelines for preventing the onset of type 2 diabetes:[citation needed]
- Healthy diet (a diet with limited refined carbohydrates, added sugars, trans fats, as well as limited intake of sodium and total calories)
- Physical fitness (30–45 minutes of cardiovascular exercise per day, 3–5 days a week)
- Weight loss by as little as 5–10 percent may have a significant impact on overall health
Management
[edit]Prediabetes is a curable disease state, and people can routinely return to normoglycemia (normal glucose metabolism) with interventions.[34] Although some drugs can delay the onset of diabetes, lifestyle modifications play a greater role in the prevention of diabetes.[15][35] Intensive weight loss and lifestyle intervention, if sustained, may improve glucose tolerance substantially and prevent progression from IGT to type 2 diabetes. The Diabetes Prevention Program (DPP)[36] study found a 16% reduction in diabetes risk for every kilogram of weight loss. Reducing weight by 7% through a low-fat diet and performing 150 minutes of exercise a week is the goal. The ADA guidelines recommend modest weight loss (5–10% body weight), moderate-intensity exercise (30 minutes daily), and smoking cessation.[37]
There are many dietary approaches that can reduce the risk of progression to diabetes. Most involve the reduction of added sugars and fats but there remains a lack of conclusive evidence proving the best approach.[38]
For patients with severe risk factors, prescription medication may be appropriate. The American Diabetes Association recommends that prescription medications may be considered for those with prediabetes, including those in a specific subgroup who are more likely to have a greater benefit from medications and are at a higher risk of progressing to diabetes. This subgroup of people includes those with a BMI greater than 35, age less than 60, women with a history of gestational diabetes, a fasting plasma glucose greater than 110 or an A1c greater than 6%.[7] This may also be considered in patients for whom lifestyle therapy has failed, or is not sustainable, who are at high-risk for developing type 2 diabetes, or who prefer to take a medication.[39] Metformin[40] and acarbose help prevent the development of prediabetes, and also have a good safety profile. Evidence also supports thiazolidinediones but there are safety concerns, and data on newer agents such as GLP-1 receptor agonists, DPP4 inhibitors or meglitinides are lacking.[41]
Prognosis
[edit]The progression to type 2 diabetes mellitus is not inevitable for those with prediabetes. The progression into diabetes mellitus from prediabetes is approximately 25% over three to five years.[42] This increases to 50% risk of progressing to diabetes over 10 years. Diabetes is a leading cause of morbidity and mortality. Effects of the disease may affect larger blood vessels (e.g., atherosclerosis within the larger arteries of the cardiovascular system) or smaller blood vessels, as seen with damage to the retina of the eye, damage to the kidney, and damage to the nerves.[9]
Prediabetes is a risk factor for mortality and there is evidence of cardiovascular disease developing prior to a diagnosis of diabetes.[43]
Epidemiology
[edit]The prevalence of prediabetes worldwide is expected to increase. In 2021 720 million people worldwide had prediabetes, and this is estimated to increase to 1 billion people by 2045.[7] Other sources estimate that the worldwide prevalence of prediabetes will increase to 11% by 2045.[7] In the United States, 38% of all adults have prediabetes.[7] In the United States, the prevalence rates of prediabetes are similar across ethnicities.[7]
The incidence of diabetes is also growing. In 2014, 29.1 million people or 9% of the US population had diabetes.[44] In 2011–2012, the prevalence of diabetes in the U.S. using hemoglobin A1C, fasting plasma glucose or the two-hour plasma glucose definition was 14% for total diabetes, 9% for diagnosed diabetes, 5% for undiagnosed diabetes and 38% for prediabetes.[45]
Research directions
[edit]Use of Continuous Glucose Monitoring
[edit]The clinical role of continuous glucose monitoring is unclear. Comparing results of CGM studies is problematic as there is a non-standardised approach towards various study parameters. The IFCC supported a review to provide recommendations that encourage the development of a standard for designing CGM performance studies, with a view to improve the clarity of their results. This standardisation is considered necessary as CGMs are becoming an increasingly indispensable tool for managing diabetes.[46]
See also
[edit]References
[edit]- ^ American Diabetes Association (January 2017). "2. Classification and Diagnosis of Diabetes". Diabetes Care. 40 (Suppl 1): S11–S24. doi:10.2337/dc17-S005. PMID 27979889.
- ^ Bennasar-Veny M, Fresneda S, López-González A, Busquets-Cortés C, Aguiló A, Yañez AM (May 2020). "Lifestyle and Progression to Type 2 Diabetes in a Cohort of Workers with Prediabetes". Nutrients. 12 (5): 1538. doi:10.3390/nu12051538. PMC 7284825. PMID 32466178.
- ^ "Do you have prediabetes? Here are the signs". American Medical Association. 12 March 2015. Retrieved 4 October 2020.
- ^ "Diabetes: 'Prediabetes'". Mayo Clinic. Retrieved January 27, 2009.
- ^ a b Wilson ML (December 2017). "Prediabetes: Beyond the Borderline". The Nursing Clinics of North America. 52 (4): 665–677. doi:10.1016/j.cnur.2017.07.011. PMID 29080583.
- ^ a b Poltavskiy E, Kim DJ, Bang H (August 2016). "Comparison of screening scores for diabetes and prediabetes". Diabetes Research and Clinical Practice. 118: 146–53. doi:10.1016/j.diabres.2016.06.022. PMC 4972666. PMID 27371780.
- ^ a b c d e f Echouffo-Tcheugui, Justin B.; Perreault, Leigh; Ji, Linong; Dagogo-Jack, Sam (11 April 2023). "Diagnosis and Management of Prediabetes: A Review". JAMA. 329 (14): 1206–1216. doi:10.1001/jama.2023.4063. PMID 37039787. S2CID 258062839.
- ^ Dietrich S, Jacobs S, Zheng JS, Meidtner K, Schwingshackl L, Schulze MB (November 2019). "Gene-lifestyle interaction on risk of type 2 diabetes: A systematic review". Obesity Reviews. 20 (11): 1557–1571. doi:10.1111/obr.12921. PMC 8650574. PMID 31478326.
- ^ a b Cotran; Kumar; Collins (1999). Robbins Pathologic Basis of Disease (Saunders Sixth ed.). pp. 913–26.
- ^ a b c American Diabetes Association (January 2019). "2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2019". Diabetes Care. 42 (Suppl 1): S13–S28. doi:10.2337/dc19-S002. PMID 30559228.
- ^ Nichols GA, Hillier TA, Brown JB (February 2007). "Progression from newly acquired impaired fasting glusose to type 2 diabetes". Diabetes Care. 30 (2): 228–33. doi:10.2337/dc06-1392. PMC 1851903. PMID 17259486.
- ^ a b "Diagnosis | ADA". diabetes.org. Retrieved 2023-09-05.
- ^ a b World Health Organization. "Definition, diagnosis and classification of diabetes mellitus and its complications: Report of a WHO Consultation. Part 1. Diagnosis and classification of diabetes mellitus". Archived from the original on June 30, 2004. Retrieved 2007-05-29.
- ^ a b American Diabetes Association (January 2005). "Diagnosis and classification of diabetes mellitus". Diabetes Care. 28 (Suppl 1): S37-42. doi:10.2337/diacare.28.suppl_1.s37. PMID 15618111.
- ^ a b Rao SS, Disraeli P, McGregor T (April 2004). "Impaired glucose tolerance and impaired fasting glucose". American Family Physician. 69 (8): 1961–8. PMID 15117017.
- ^ a b c Lima LM (May 2017). "Subclinical Diabetes". Anais da Academia Brasileira de Ciências. 89 (1): 591–614. doi:10.1590/0001-3765201720160394. PMID 28492735.
- ^ Kraft JR (1975). "Detection of Diabetes Mellitus In Situ (Occult Diabetes)". Laboratory Medicine. 6 (2): 10–22. doi:10.1093/labmed/6.2.10.
- ^ Reaven GM, Lerner RL, Stern MP, Farquhar JW (November 1967). "Role of insulin in endogenous hypertriglyceridemia". The Journal of Clinical Investigation. 46 (11): 1756–67. doi:10.1172/JCI105666. PMC 292926. PMID 6061748.
- ^ "Consensus Development Conference on Insulin Resistance. 5-6 November 1997. American Diabetes Association". Diabetes Care. 21 (2): 310–4. February 1998. doi:10.2337/diacare.21.2.310. PMID 9540000. S2CID 11145582.
- ^ Keebler ME, McGuire DK (August 2003). "Subclinical diabetes mellitus: is it really "sub-clinical"?". American Heart Journal. 146 (2): 210–2. doi:10.1016/S0002-8703(03)00236-9. PMID 12891185.
- ^ Lima LM (February 2017). "Prediabetes definitions and clinical outcomes". The Lancet. Diabetes & Endocrinology. 5 (2): 92–93. doi:10.1016/S2213-8587(17)30011-6. PMID 28129828.
- ^ Hanley AJ, Williams K, Stern MP, Haffner SM (July 2002). "Homeostasis model assessment of insulin resistance in relation to the incidence of cardiovascular disease: the San Antonio Heart Study". Diabetes Care. 25 (7): 1177–84. doi:10.2337/diacare.25.7.1177. PMID 12087016.
- ^ Valenti V, Hartaigh BÓ, Cho I, Schulman-Marcus J, Gransar H, Heo R, et al. (February 2016). "Absence of Coronary Artery Calcium Identifies Asymptomatic Diabetic Individuals at Low Near-Term But Not Long-Term Risk of Mortality: A 15-Year Follow-Up Study of 9715 Patients". Circulation: Cardiovascular Imaging. 9 (2): e003528. doi:10.1161/CIRCIMAGING.115.003528. PMC 4745994. PMID 26848062.
- ^ The Decode Study Group (March 2003). "Is the current definition for diabetes relevant to mortality risk from all causes and cardiovascular and noncardiovascular diseases?". Diabetes Care. 26 (3): 688–96. doi:10.2337/diacare.26.3.688. PMID 12610023.
- ^ "ADA: Standards of Medical Care in Diabetes", Diabetes Care 27: Supp 1.515, 2004.
- ^ "Diabetes Guidelines Taskforce: AACE Guidelines for the Management of DM", Endocrin Pract 1995, 1.149
- ^ Abid A, Ahmad S, Waheed A (January 2016). "Screening for Type II Diabetes Mellitus in the United States: The Present and the Future". Clinical Medicine Insights. Endocrinology and Diabetes. 9: 19–22. doi:10.4137/CMED.S38247. PMC 4907337. PMID 27330335.
- ^ "Diabetes: putting people at the heart of services". NIHR Evidence. 2022-07-26. doi:10.3310/nihrevidence_52026. S2CID 251299176.
- ^ "Are you at risk of diabetes? Research finds prevention should start at a different BMI for each ethnic group". NIHR Evidence. 2022-03-10. doi:10.3310/alert_48878. S2CID 247390548.
- ^ Caleyachetty R, Barber TM, Mohammed NI, Cappuccio FP, Hardy R, Mathur R, et al. (July 2021). "Ethnicity-specific BMI cutoffs for obesity based on type 2 diabetes risk in England: a population-based cohort study". The Lancet. Diabetes & Endocrinology. 9 (7): 419–426. doi:10.1016/S2213-8587(21)00088-7. PMC 8208895. PMID 33989535.
- ^ Strachan SM, Bean C, Jung ME (November 2018). "'I'm on the train and I can't stop it': Western Canadians' reactions to prediabetes and the role of self-compassion". Health & Social Care in the Community. 26 (6): 979–987. doi:10.1111/hsc.12628. hdl:2429/70654. PMID 30074658. S2CID 51907888.
- ^ "Type 2 Diabetes - Symptoms, Causes, Treatment". www.diabetes.org. Retrieved 2020-05-01.
- ^ "CDC - About the Program - National Diabetes Prevention Program - Diabetes DDT". www.cdc.gov. 2019-08-02. Retrieved 2020-05-01.
- ^ Eldin WS, Emara M, Shoker A (April 2008). "Prediabetes: a must to recognise disease state". International Journal of Clinical Practice. 62 (4): 642–8. doi:10.1111/j.1742-1241.2008.01705.x. PMID 18266711. S2CID 22360799.
- ^ Raina Elley C, Kenealy T (December 2008). "Lifestyle interventions reduced the long-term risk of diabetes in adults with impaired glucose tolerance". Evidence-Based Medicine. 13 (6): 173. doi:10.1136/ebm.13.6.173. PMID 19043031. S2CID 26714233.
- ^ "Diabetes Prevention Program (DPP)". 31 August 2021.
- ^ American Diabetes Association. "How to Prevent or Delay Diabetes". Archived from the original on 2009-08-22.
- ^ Taubes G (27 December 2017). "Minimal carbs, lots of fat, incredible dieting results – but not enough science". Retrieved 2018-03-24.
- ^ UptoDate: Prediction and prevention of type 2 diabetes mellitus; www.utdol.com/utd/content/topic.do?topicKey=diabetes.
- ^ Lily M, Lilly M, Godwin M (April 2009). "Treating prediabetes with metformin: systematic review and meta-analysis". Canadian Family Physician. 55 (4): 363–9. PMC 2669003. PMID 19366942.
- ^ "American College of Endocrinology Consensus Statement on the diagnosis and management of pre-diabetes in the continuum of hyperglycemia – When do the risks of diabetes begin?" (PDF). American College of Endocrinology Task Force on Pre-Diabetes. Retrieved 2008-07-24.
- ^ Nathan DM, Davidson MB, DeFronzo RA, Heine RJ, Henry RR, Pratley R, Zinman B (March 2007). "Impaired fasting glucose and impaired glucose tolerance: implications for care". Diabetes Care. 30 (3): 753–9. doi:10.2337/dc07-9920. PMID 17327355.
- ^ Barr EL, Zimmet PZ, Welborn TA, Jolley D, Magliano DJ, Dunstan DW, et al. (July 2007). "Risk of cardiovascular and all-cause mortality in individuals with diabetes mellitus, impaired fasting glucose, and impaired glucose tolerance: the Australian Diabetes, Obesity, and Lifestyle Study (AusDiab)". Circulation. 116 (2): 151–7. doi:10.1161/CIRCULATIONAHA.106.685628. hdl:10536/DRO/DU:30020817. PMID 17576864.
- ^ Centers for Disease Control and Prevention (2014). "National Diabetes Statistics Report: Estimates of Diabetes and its Burden in the United States, 2014". Atlanta, GA: U.S. Department of Health and Human Services. Archived from the original on 2016-12-02.
- ^ Menke A, Casagrande S, Geiss L, Cowie CC (September 2015). "Prevalence of and Trends in Diabetes Among Adults in the United States, 1988-2012". JAMA. 314 (10): 1021–9. doi:10.1001/jama.2015.10029. PMID 26348752.
- ^ Freckmann G, Eichenlaub M, Waldenmaier D, Pleus S, Wehrstedt S, Haug C, Witthauer L, Jendle J, Hinzmann R, Thomas A, Eriksson Boija E, Makris K, Diem P, Tran N, Klonoff DC, Nichols JH, Slingerland RJ (August 2023). "Clinical Performance Evaluation of Continuous Glucose Monitoring Systems: A Scoping Review and Recommendations for Reporting". J Diabetes Sci Technol. 17 (6): 1506–1526. doi:10.1177/19322968231190941. PMC 10658695. PMID 37599389.
Further reading
[edit]- Davies MJ, Gray IP (February 1996). "Impaired glucose tolerance". BMJ. 312 (7026): 264–5. doi:10.1136/bmj.312.7026.264. PMC 2349870. PMID 8611769. – Editorial review
- Nathan DM, Davidson MB, DeFronzo RA, Heine RJ, Henry RR, Pratley R, Zinman B (March 2007). "Impaired fasting glucose and impaired glucose tolerance: implications for care". Diabetes Care. 30 (3): 753–9. doi:10.2337/dc07-9920. PMID 17327355.